
Neonatal Neurology 4
Session: Neonatal Neurology 4
 photo")
Emily W.Y Tam, MDCM, MAS, FRCPC (she/her/hers)
Associate Professor
The Hospital for Sick Children
Toronto, Ontario, Canada
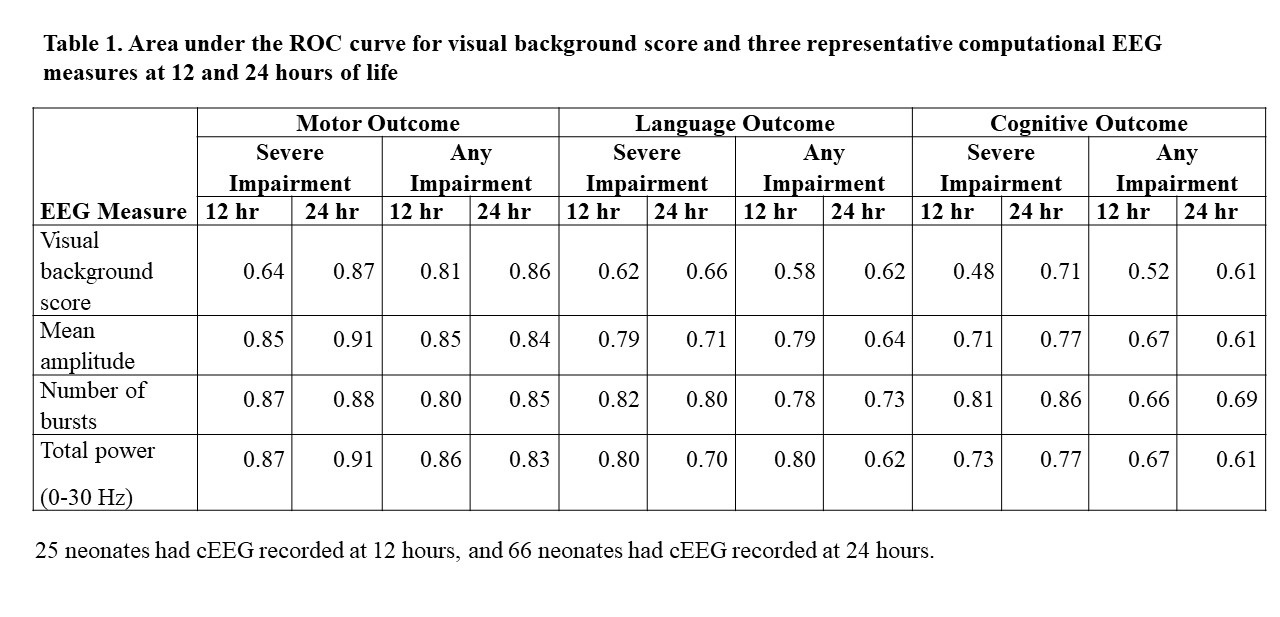 Area under the ROC curve for visual background score and three representative computational EEG measures at 12 and 24 hours of life
Area under the ROC curve for visual background score and three representative computational EEG measures at 12 and 24 hours of life