457 - An Extension for Community Healthcare Outcomes (ECHOTM) Model of Lead Poisoning Prevention Educational Outreach & Quality Improvement: The New Hampshire Experience.
Sunday, April 27, 2025
8:30am - 10:45am HST
Publication Number: 457.3622
Alan D. Woolf, Boston Children's Hospital, Boston, MA, United States; Gail Gettens, NH DHHS Division of Public Health Services, Concord, NH, United States; Nicole Lang, NH Department of Health and Human Services, Division of Public Health, Concord, NH, United States; Ruth S. Gubernick, RSG Consulting, Collingswood, NJ, United States
Senior Associate in Pediatrics Boston Children's Hospital Boston, Massachusetts, United States
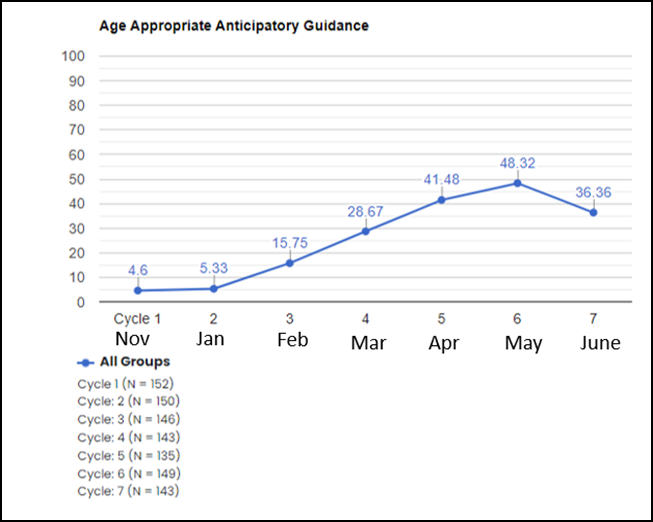
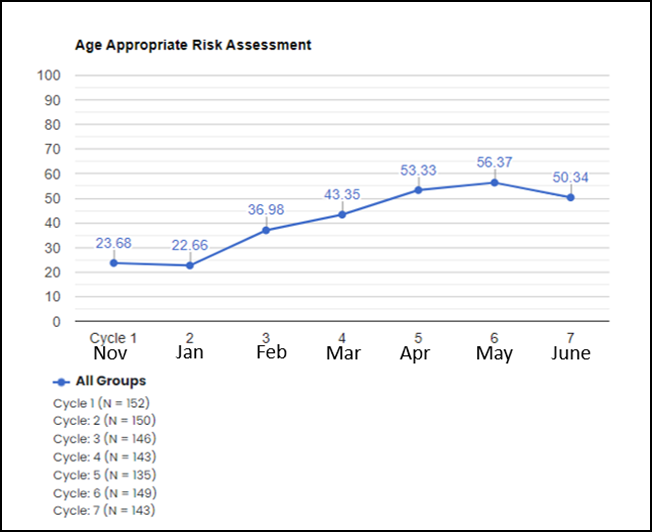
Background: The ECHO(TM) format of professional education, a “hub-and-spoke” model of educational outreach developed by the U. of New Mexico, has been implemented for many pediatric topics. The model was adopted by the NH Department of Health & Human Services, Division of Public Health Services to address a post-pandemic decline in pediatric lead testing at ages 1 & 2, as mandated by state law in 2018. Support was obtained from non-profits, including managed care organization AmeriHealth Caritas NH, NH Chapter of the American Academy of Pediatrics, and Region 1 Pediatric Environmental Health Specialty Unit. Objective: Practices were enrolled in an educational lead testing initiative with a quality improvement component to investigate whether this intervention could change rates of risk assessment and anticipatory guidance. Design/Methods: Practices were solicited via email in 2023 to join the 6-session, virtual ECHO(TM), conducted January-June 2024. At each session, content experts delivered 10-minute presentations. Practices submitted clinical cases presented monthly. This ECHO(TM) included a quality improvement component requiring practices to submit data monthly; 7 cycles of data were analyzed and presented at sessions. Pediatricians earned 25 Maintenance of Certification Part 4 credits. The Chi square statistic (with Yates correction; alpha = 0.05) was used to determine statistical significance. Results: Eight practice teams (38 individuals) participated. Practices reported rates of anticipatory guidance and lead risk assessment monthly, auditing up to 20 encounters for 6-24 month Well Child visits. Practices also reported monthly rates of lead testing performed for all 12 and 24 month Well Child visits. Results showed a trend towards improvement. Age-appropriate risk assessment improved from 23.68% to 50.34% (X2=6.8353; p=0.0089); anticipatory guidance on lead poisoning prevention improved from 4.6% to 36.36% (X2=21.1871; p< 0.00001); lead testing of 1-year-olds improved from 81.41% to 89.49% (X2=2.045; p=0.1527); lead testing of 2-year-olds improved from 74.38% to 76.53% (X2=0.0439; p=0.8341).
Conclusion(s): Practices enrolled in a NH educational lead testing initiative with a quality improvement component showed a significant increase in rates of risk assessment and anticipatory guidance. A positive impact on lead testing rates was also noted, although it did not achieve significance, likely due to small sample size. Clinical staff demonstrated willingness to modify practices to support care. The ECHO(TM) model can make a positive impact on pediatric lead testing rates and prevention of lead poisoning.

 Credit")
 photo")