
Newborn Care 1
Session: Newborn Care 1
 Credit")

Oresta Rule, MD
Assistant Professor
University of Wisconsin School of Medicine and Public Health
Madison, Wisconsin, United States
.jpg) Control charts from 11/1/23-9/17/24 demonstrate a decrease in the biweekly proportion of late preterm and early term singleton infants receiving supplemental formula at hospital discharge and 2-week visit after initiation of a DHM voucher program: supplemental formula use decreased from 58.2% to 28.2% (-30.0p.p.) at hospital discharge and from 38.5% to 24.8% (-13.7p.p.) at 2-week visit. The proportion of infants receiving supplemental formula during birth admission remained unchanged at 31.5%.
Control charts from 11/1/23-9/17/24 demonstrate a decrease in the biweekly proportion of late preterm and early term singleton infants receiving supplemental formula at hospital discharge and 2-week visit after initiation of a DHM voucher program: supplemental formula use decreased from 58.2% to 28.2% (-30.0p.p.) at hospital discharge and from 38.5% to 24.8% (-13.7p.p.) at 2-week visit. The proportion of infants receiving supplemental formula during birth admission remained unchanged at 31.5%.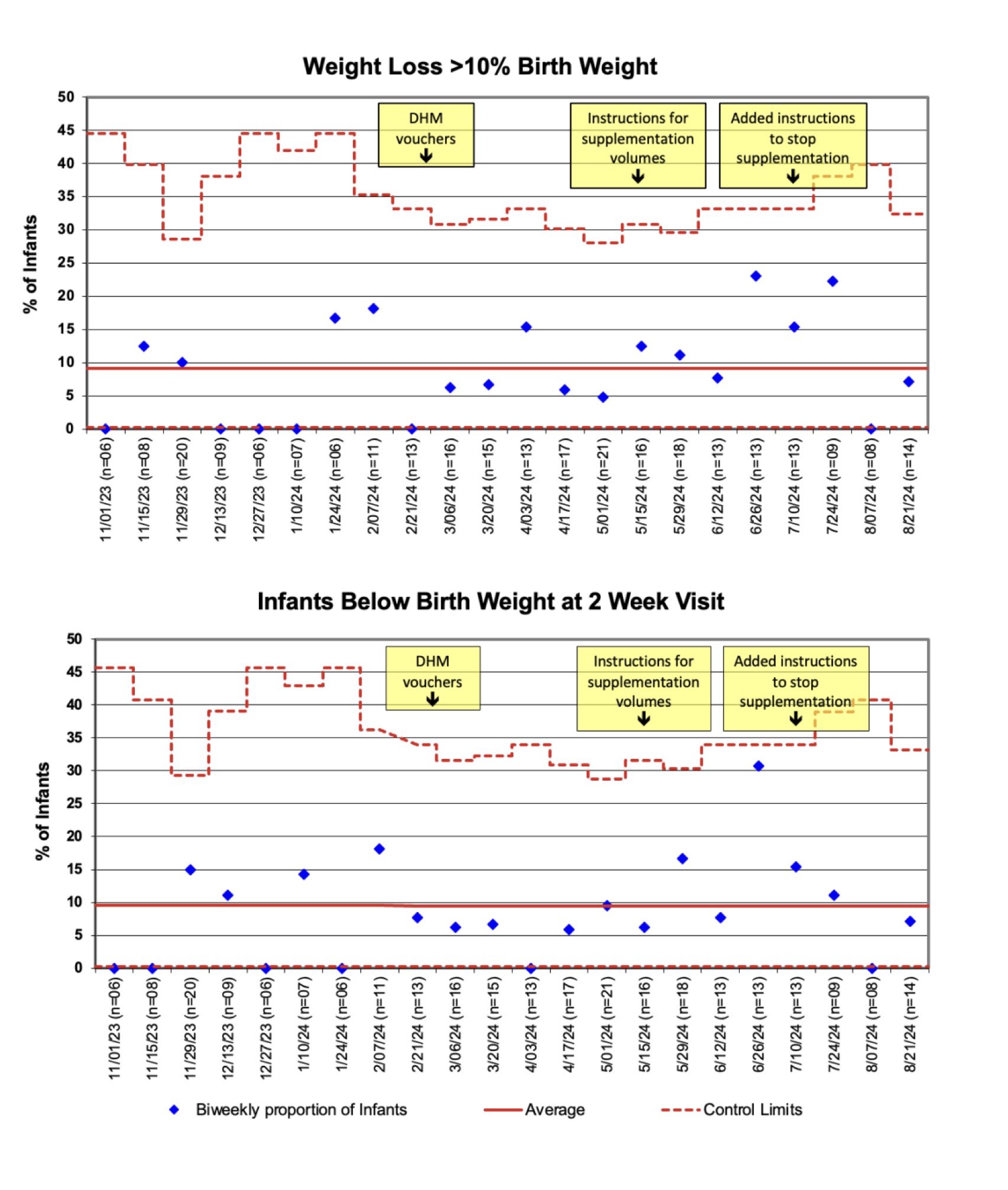 Control charts from 11/1/23-9/17/24 show no change in biweekly proportion of late preterm and early term singleton infants with excessive weight loss (>10% of birth weight) or failure to regain birth weight by 2-week visit.Control charts from 11/1/23-9/17/24 demonstrate a decrease in the biweekly proportion of late preterm and early term singleton infants receiving supplemental formula at hospital discharge and 2-week visit after initiation of a DHM voucher program: supplemental formula use decreased from 58.2% to 28.2% (-30.0p.p.) at hospital discharge and from 38.5% to 24.8% (-13.7p.p.) at 2-week visit. The proportion of infants receiving supplemental formula during birth admission remained unchanged at 31.5%.Control charts from 11/1/23-9/17/24 show no change in biweekly proportion of late preterm and early term singleton infants with excessive weight loss (>10% of birth weight) or failure to regain birth weight by 2-week visit.
Control charts from 11/1/23-9/17/24 show no change in biweekly proportion of late preterm and early term singleton infants with excessive weight loss (>10% of birth weight) or failure to regain birth weight by 2-week visit.Control charts from 11/1/23-9/17/24 demonstrate a decrease in the biweekly proportion of late preterm and early term singleton infants receiving supplemental formula at hospital discharge and 2-week visit after initiation of a DHM voucher program: supplemental formula use decreased from 58.2% to 28.2% (-30.0p.p.) at hospital discharge and from 38.5% to 24.8% (-13.7p.p.) at 2-week visit. The proportion of infants receiving supplemental formula during birth admission remained unchanged at 31.5%.Control charts from 11/1/23-9/17/24 show no change in biweekly proportion of late preterm and early term singleton infants with excessive weight loss (>10% of birth weight) or failure to regain birth weight by 2-week visit.