
Nephrology 4
Session: Nephrology 4
.jpeg.jpg "Rayan Terkawi, MD (MBBS) photo")
Rayan Terkawi, MD (MBBS)
Pediatric Nephrology Fellow
University of Miami/ Jackson Health System
Miami, Florida, United States
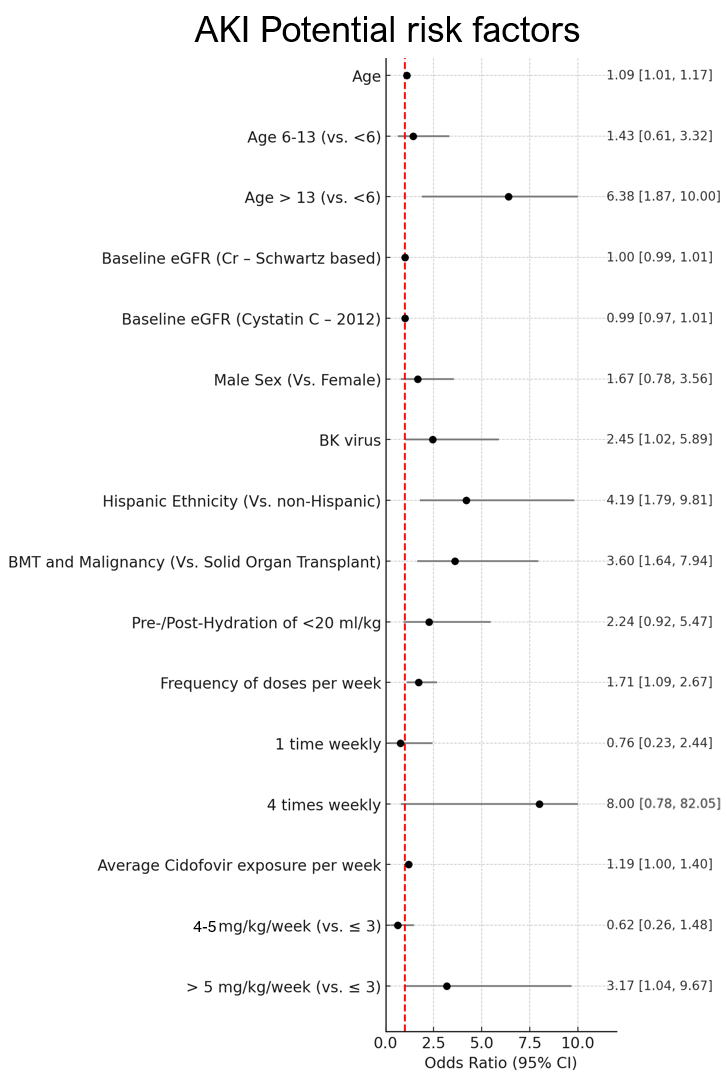 Forest plot showing risk factors for AKI in immunocompromised patients treated with cidofovir
Forest plot showing risk factors for AKI in immunocompromised patients treated with cidofovir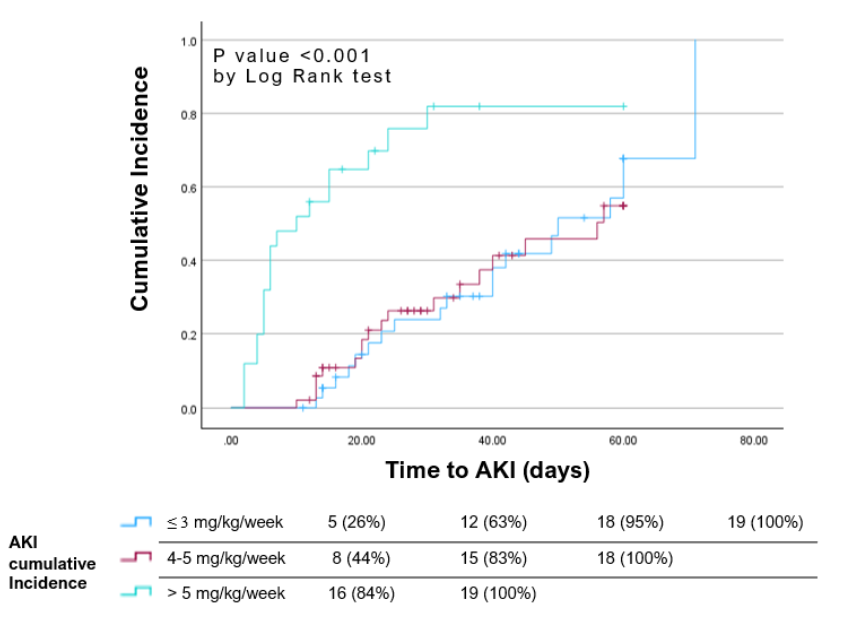 Kaplan–Meier plot showing time to AKI event by weekly cidofovir dosing regimen
Kaplan–Meier plot showing time to AKI event by weekly cidofovir dosing regimen