
Newborn Care 1
Session: Newborn Care 1
 photo")
Kendall Steadmon, MD (she/her/hers)
Clinical Associate Professor
University of Florida College of Medicine
Micanopy, Florida, United States
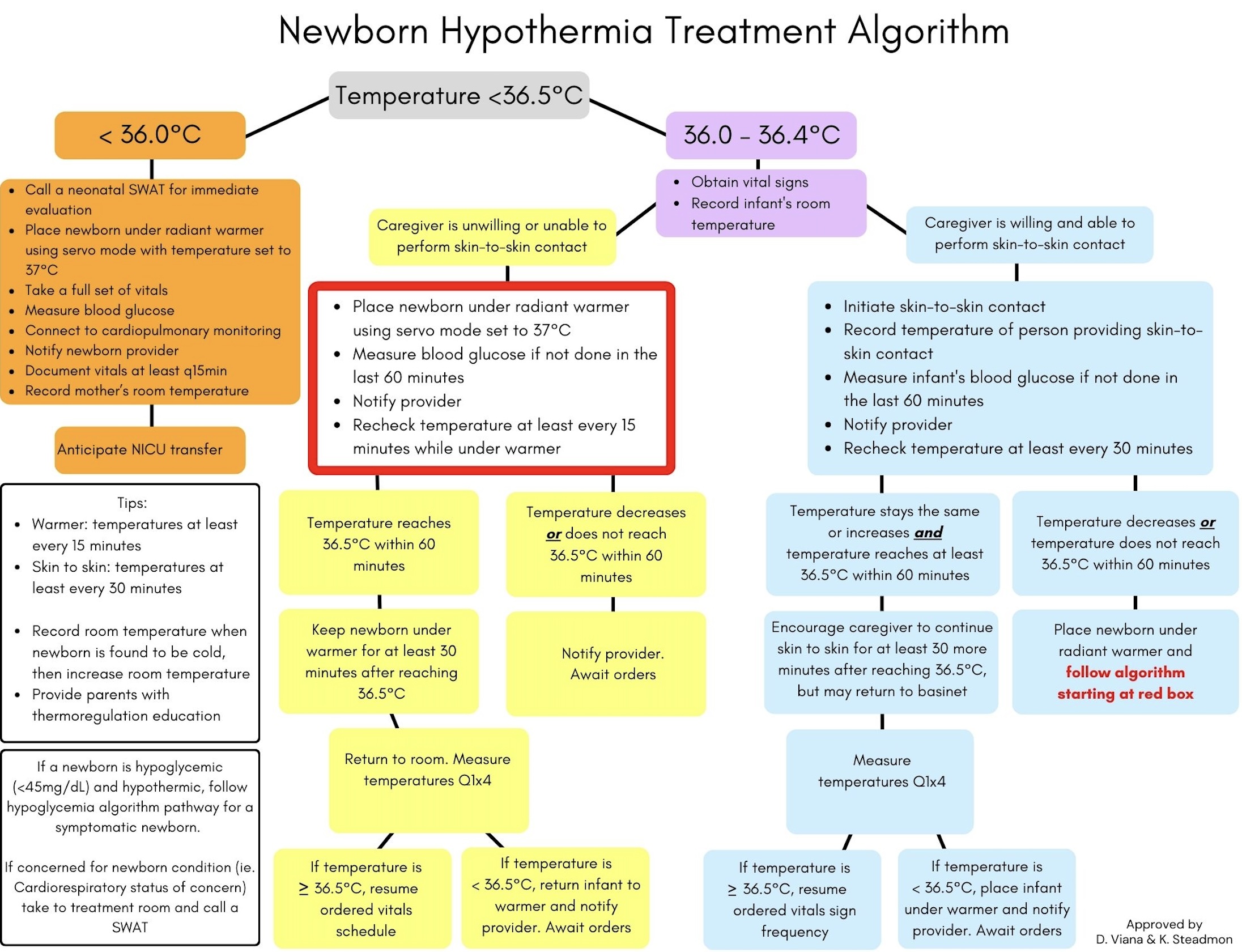 Example of the newborn hypothermia treatment algorithm implemented in the QI project.
Example of the newborn hypothermia treatment algorithm implemented in the QI project.