
Nephrology 6
Session: Nephrology 6
 photo")
Alexis C. Gomez, MD (she/her/hers)
Fellow
Boston Children's Hospital
West Roxbury, Massachusetts, United States
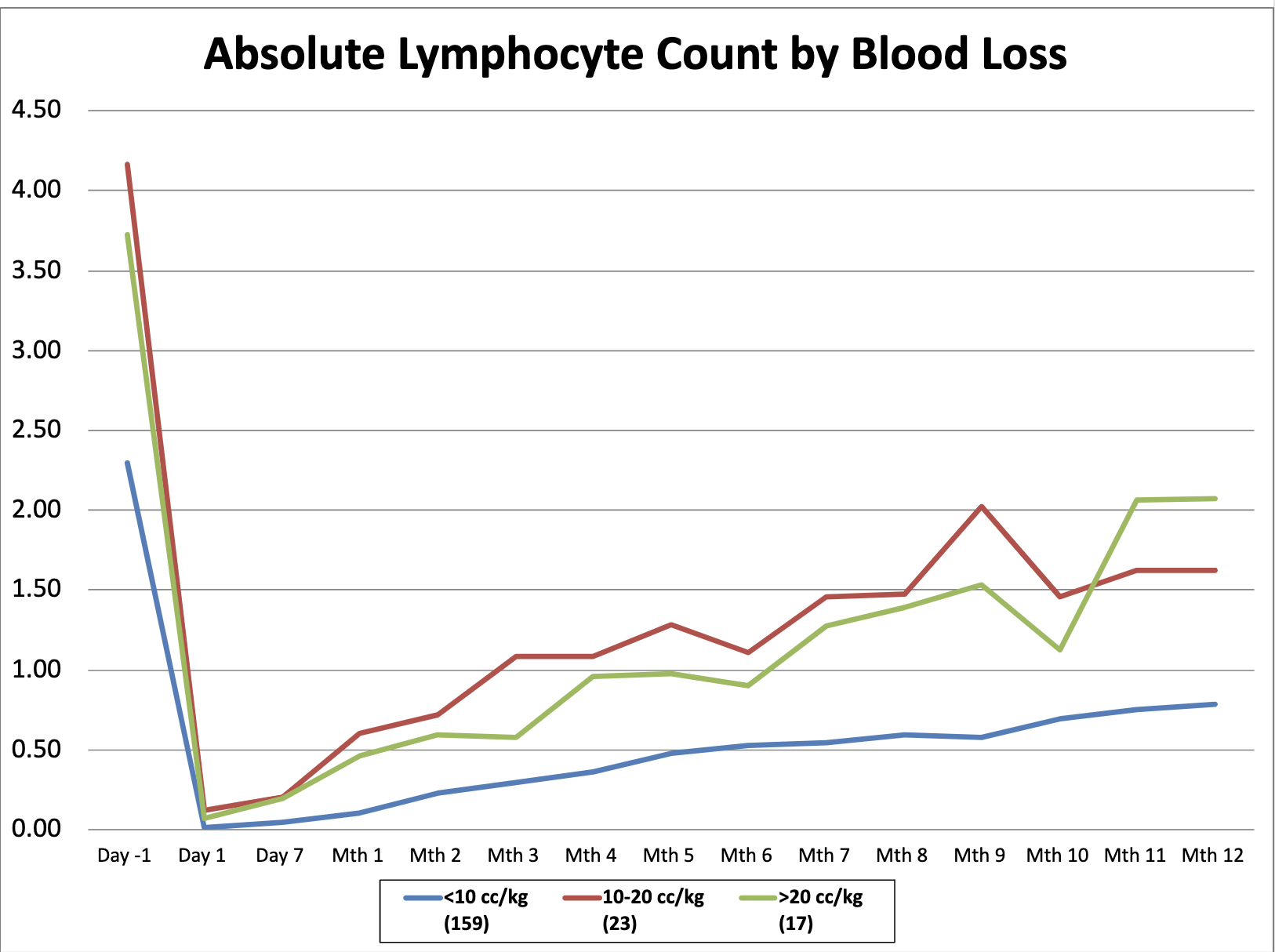 lymphocyte repopulation over the first 12 months post transplant stratified by degree of blood loss
lymphocyte repopulation over the first 12 months post transplant stratified by degree of blood loss 