
Nephrology 2
Session: Nephrology 2
Tyler Shimfessel, MD
Resident
University of Texas Southwestern Medical School
Dallas, Texas, United States
.png)
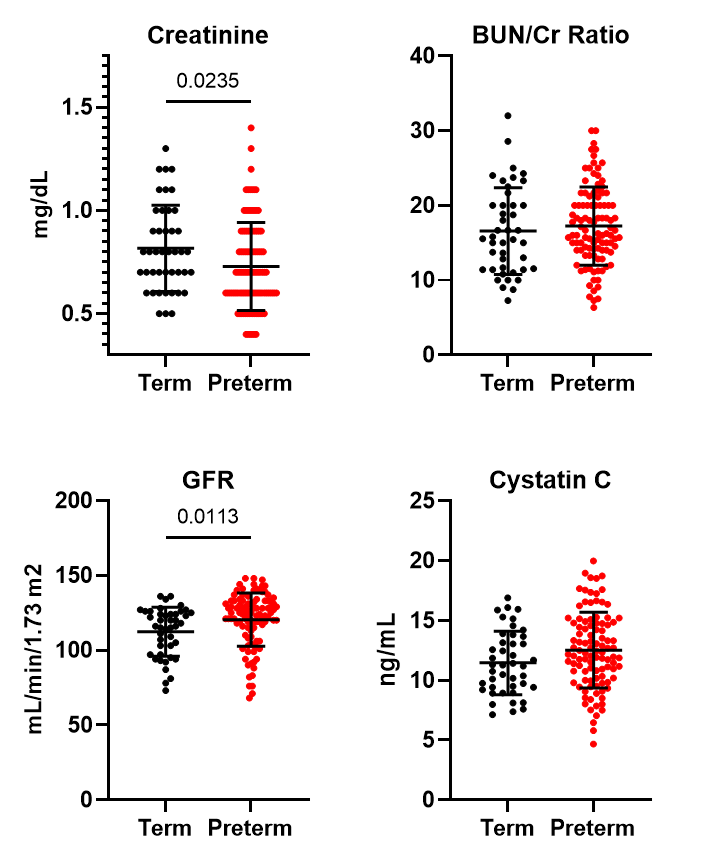 Adolescents and adults born prematurely exhibit reduced Creatinine (p=0.024) and higher Glomerular Filtration Rate (GFR) (p=0.011) compared to term-born participants.
Adolescents and adults born prematurely exhibit reduced Creatinine (p=0.024) and higher Glomerular Filtration Rate (GFR) (p=0.011) compared to term-born participants.