
Infectious Diseases 5: In utero exposures and infections
Session: Infectious Diseases 5: In utero exposures and infections
 photo")
Dylan Brown, BS (he/him/his)
Research Assistant
Nationwide Children's Hospital
Columbus, Ohio, United States
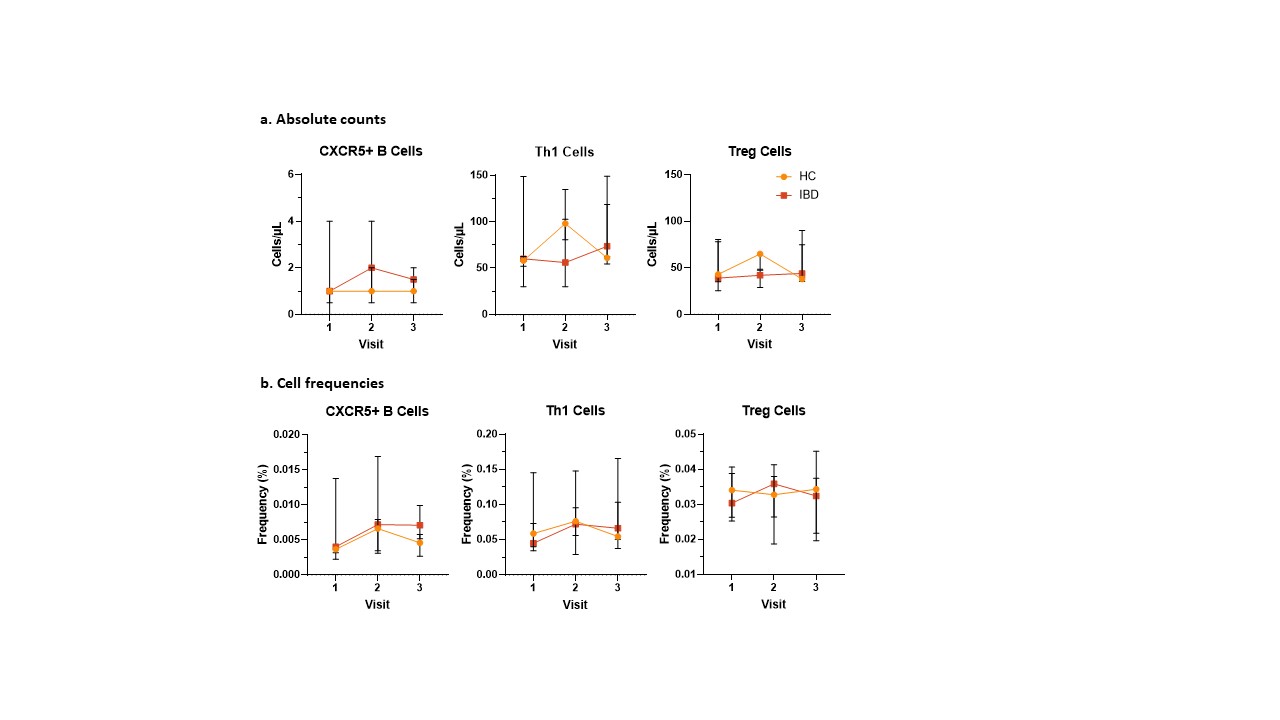 Changes in cell populations after influenza vaccination
Changes in cell populations after influenza vaccination