
Nephrology 6
Session: Nephrology 6
 photo")
Elizabeth Rivas, MD (she/her/hers)
Pediatric Nephrology Second Year Fellow
University of Miami Leonard M. Miller School of Medicine
Miami, Florida, United States
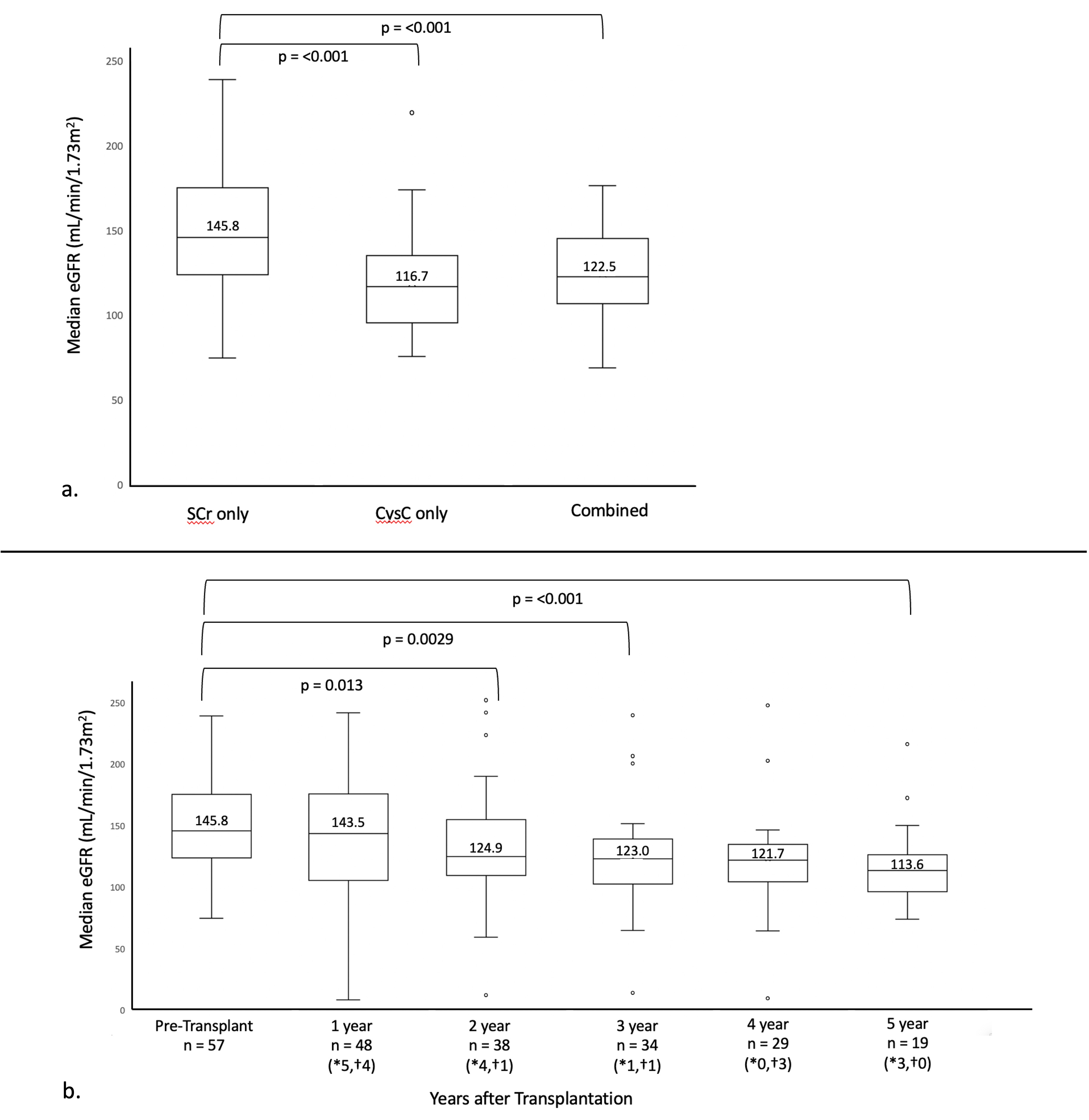 a. eGFR by SCr alone (Bedside Schwartz formula) compared to CysC alone (CKiD U25 formula) and combined (CKiD U25 formula) b. Trend in median SCr eGFR over time post-transplant; *number of patients removed from analysis due to death, †number of patients removed from analysis due to graft failure
a. eGFR by SCr alone (Bedside Schwartz formula) compared to CysC alone (CKiD U25 formula) and combined (CKiD U25 formula) b. Trend in median SCr eGFR over time post-transplant; *number of patients removed from analysis due to death, †number of patients removed from analysis due to graft failure