464 - Improving Lead Screening Rates in the Ambulatory Setting in Peoria, Illinois via Quality Improvement
Sunday, April 27, 2025
8:30am - 10:45am HST
Publication Number: 464.5480
Ishita Bhattacharya, University of Illinois College of Medicine, Peoria, IL, United States; Mary E. Bass, University of Illinois College of Medicine, Peoria, IL, United States; Anjeli Stevens, University of Illinois College of Medicine, Peoria, IL, United States; Marte Deppermann, University Pediatrics, Trivoli, IL, United States; Heather McLauchlan, University of Illinois College of Medicine, Morton, IL, United States; Jalayne M. Lapke, University of Illinois College of Medicine, Peoria, IL, United States; Kristine Papis, University of Illinois College of Medicine, Peoria, IL, United States
Medical Student University of Illinois College of Medicine Peoria, Illinois, United States
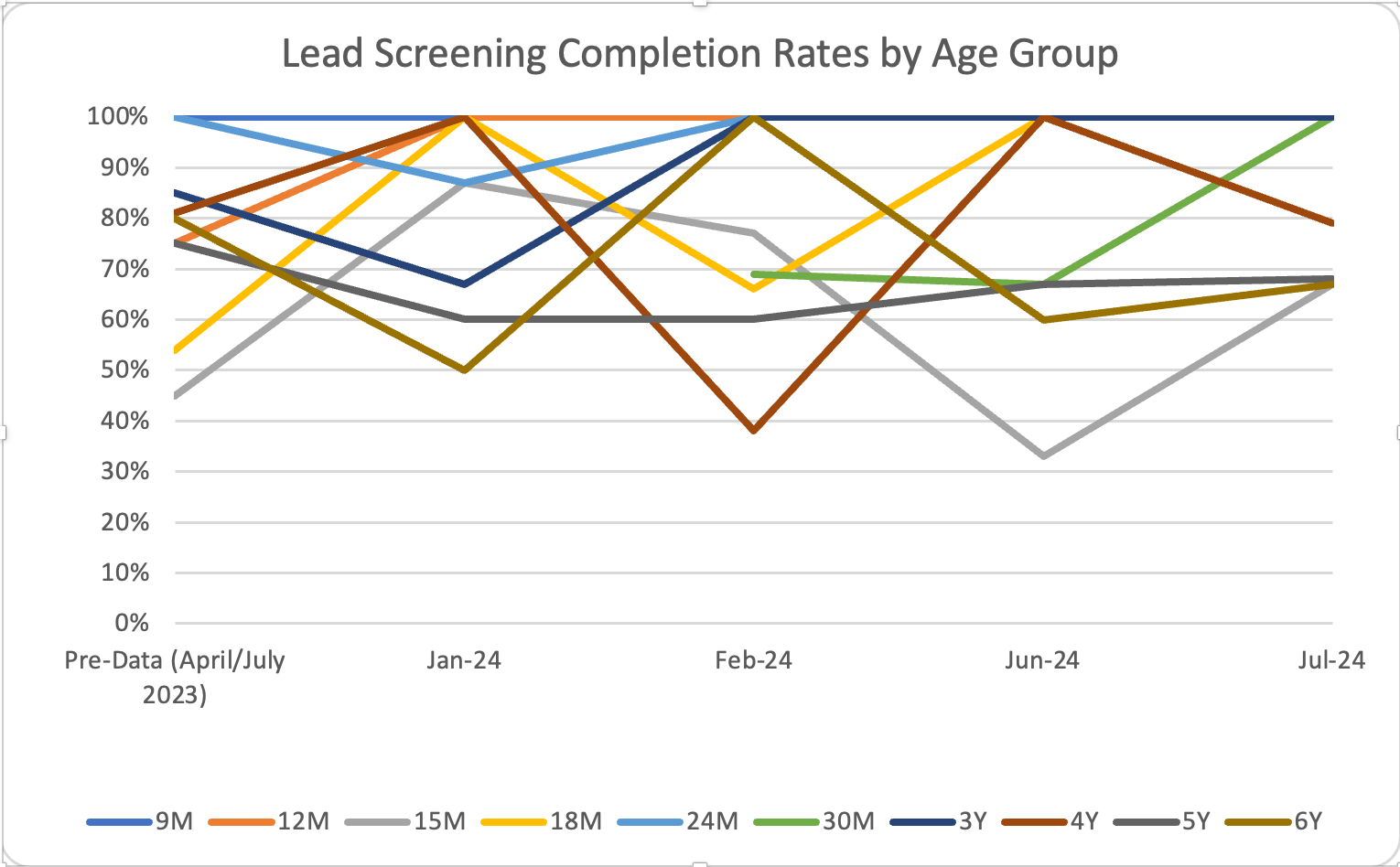
Background: Lead exposure is a risk factor for diminished intellectual abilities and higher rates of neurobehavioral disorders, such as hyperactivity and attention deficits, at any blood concentration level. Approximately 2.6% of preschool children in the United States have a blood lead concentration >5 µg/dL. In Illinois, screening for lead poisoning should be completed in children 6 years and younger, with point of care (POC) testing required for all by 1 year and repeated after 2 years of age. Approximately 13.5% of children tested in Peoria County 6 years and younger have high lead levels, compared to the 2.5% national average. Only 45% of this population has undergone lead testing at least once in their lifetime. Objective: Ensure that lead risk assessment completion for well-child checks (WCC) ages 9 months through 6 years and office compliance of point of care (POC) testing for lead at 9 months and 2 years is at a minimum rate of 90%. Design/Methods: Retrospective chart review assessed baseline data for completion of lead risk assessment screens at WCC ages 9 months to 6 years and collection of POC lead level for patients deemed high-risk. Following baseline data collection, staff underwent formalized education based on Illinois Department of Public Health guidelines on lead screening and were instructed on how to administer the risk assessment screening. Providers reviewed the assessment and informed the Certified Medical Assistant if a POC level was needed outside of the standard POC level done at 9 months and 2 year WCCs. Post-intervention data was collected to assess screening completion and standard POC compliance. Results: Baseline data showed a 74% lead risk assessment screening completion rate and an 82% POC test compliance rate. Post-intervention data showed an initial improvement in overall lead risk assessment completion to 86 % and POC compliance to 97% in the first month. Subsequent months had an average of 80% completion and 86% compliance. Analysis by age group saw notable improvements in the 12-month, 30-month, and 3-year groups, where completion rates increased to and remained at 100%.
Conclusion(s): Pediatric ambulatory sites should strive for complete lead screening to ensure children’s safety, and to contribute to emerging data that may suggest a need to lower the national blood lead reference value, as was done in 2021. Periodic guideline-based education and reminders can improve and sustain lead risk assessment screening rates to ensure high lead levels are detected and appropriately treated.

 Credit")