
Neonatal Neurology 4
Session: Neonatal Neurology 4
 photo")
Natalie L. Smith, MD (she/her/hers)
Neonatal Perinatal Medicine Fellow
University of Southern California
Los Angeles, California, United States
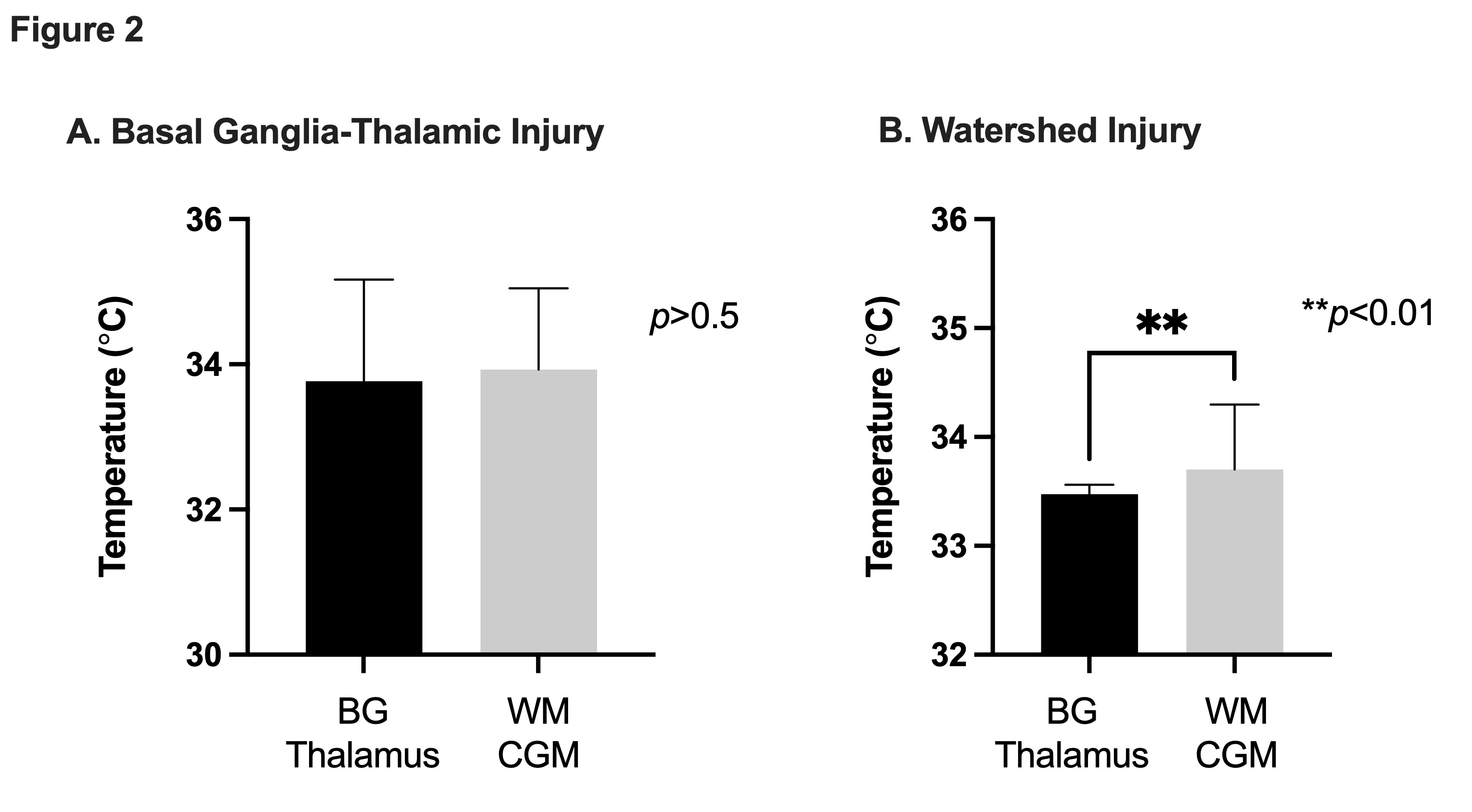 Regional brain temperatures compared to pattern of brain injury.
Regional brain temperatures compared to pattern of brain injury. 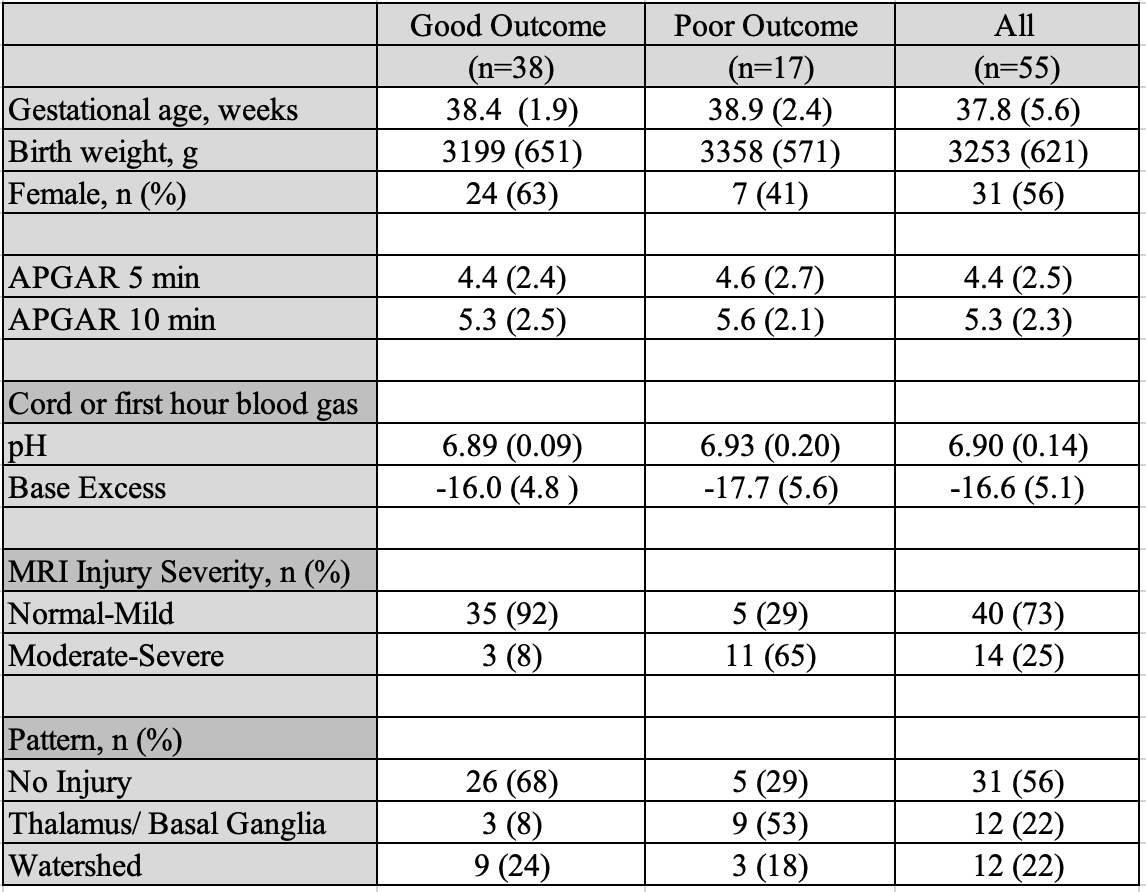 Numbers are reported as mean (standard deviation), unless specified as number (%).
Numbers are reported as mean (standard deviation), unless specified as number (%). 