
Nephrology 2
Session: Nephrology 2
 photo")
Julia W. McDonald, MD (she/her/hers)
Pediatric Nephrology Fellow
UPMC Childrens Hospital of Pittsburgh
Pittsburgh, Pennsylvania, United States
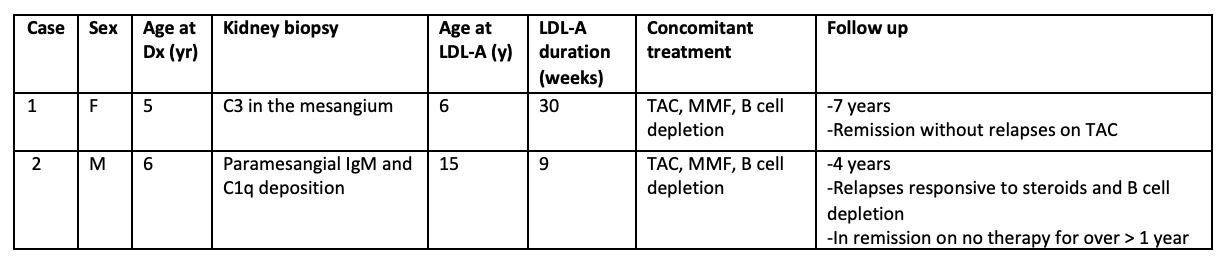 Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)
Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF).jpg) Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)
Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)Therapeutic plasma exchange (TPE), Tacrolimus (TAC), Mycophenolic acid (MMF)