130 - Oral Ibuprofen Use for Pediatric Patients with Traumatic Pain: A National Overview of 4 years of EMS Practices
Sunday, April 27, 2025
8:30am – 10:45am HST
Kathryn Kothari, Baylor College of Medicine, Houston, TX, United States; Elizabeth Camp, Baylor College of Medicine, Houston, TX, United States; Remle P.. Crowe, ESO, Austin, TX, United States; Manish I.. Shah, Stanford University School of Medicine, Palo Alto, CA, United States
Assistant Professor Baylor College of Medicine / Texas Children's Hospital Houston, Texas, United States
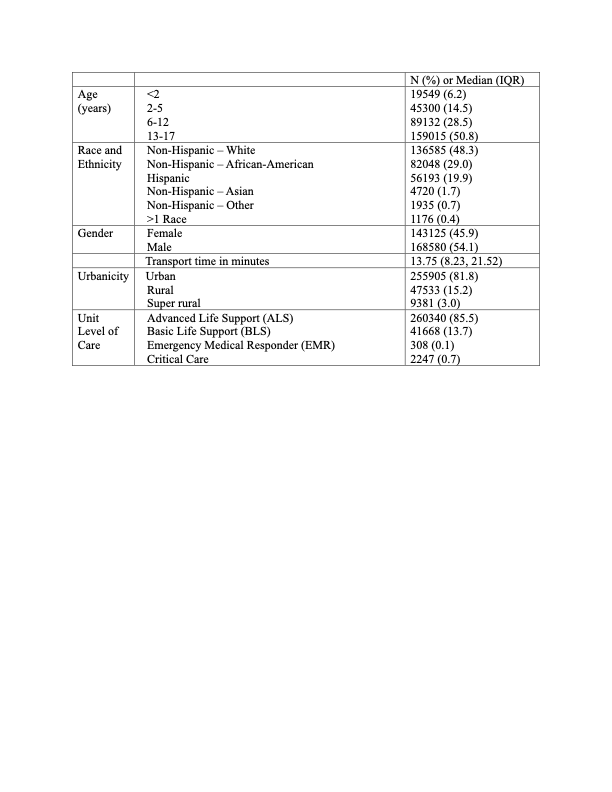
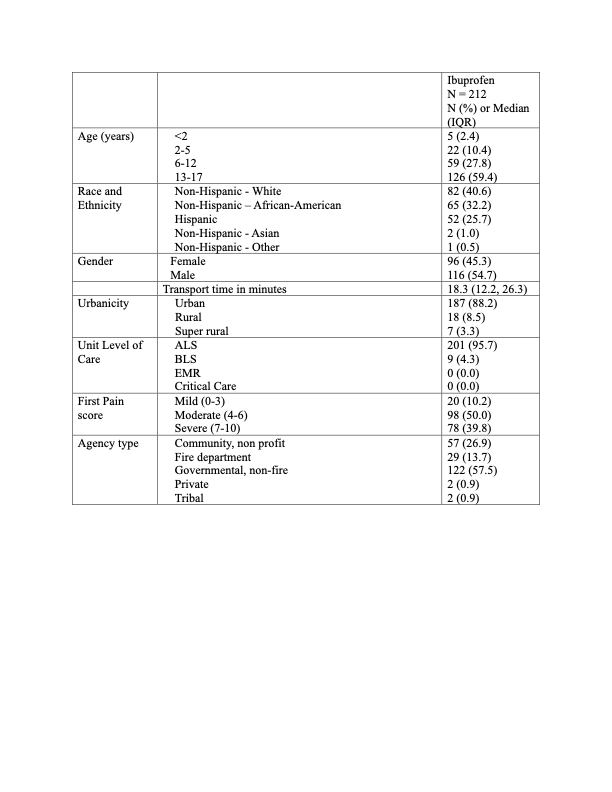
Background: Pediatric traumatic pain is undertreated in Emergency Medical Services (EMS) encounters, with barriers including concern for administering opioids to children. Ibuprofen, a safe and effective non-opioid analgesic, is commonly used in emergency departments for injured children. Little is understood about the use of ibuprofen for pain management in pediatric patients during EMS encounters. Objective: To describe national practice patterns of ibuprofen administration by EMS for children with traumatic pain. Design/Methods: This retrospective observational study from 2019-2022 used the 2022 ESO Data Collaborative, a national data set of US prehospital electronic health records. We evaluated all 911 responses of children 6 months to 17 years with an injury. Children with altered mental status, pregnancy and fever were excluded. Ibuprofen administrations prior to EMS arrival were excluded. Descriptive statistics were calculated. Pain scores (PS) were categorized as mild (PS 0-3), moderate (PS 4-6) and severe (PS 7-10). Results: 312,996 injured children were included in the study population. The age distribution was as follows: 51% (n=159,015) 13-17 years, 29% (n=89,132) 6-12 years, 15% (n=45,300) 2-5 years, and 6% (n=19,549) under 2 years (Table 1). PS were documented in 76% (n=236,639). Overall, 10% (n=30,659) of injured children received analgesics, with only 212 receiving ibuprofen. Of the children receiving ibuprofen, 12% (26/212) were under 5 years old (Table 2). The median PS for ibuprofen administration was 6 (IQR 4-8). Among those with documented moderate pain, 6% (n=4,540) received any analgesic. In contrast, children receiving fentanyl (n=25,903) had a median highest PS of 9 (IQR 8-10) (Table 3). In those receiving ibuprofen, 10% (n=20) had mild pain, 50% (n=98) had moderate pain and 40% (n=78) had severe pain. Ibuprofen was primarily administered by Advanced Life Support (96%, n=201) and in urban settings (88%, n=187). The most common injury mechanisms among ibuprofen recipients were falls (n=65), motor vehicle accidents (n=48), and assaults (n=23).
Conclusion(s): Only 1 in 10 injured children received analgesics in the prehospital setting. Despite ibuprofen being a safe and effective non-opioid analgesic, it is underutilized in the EMS setting. As untreated pain can contribute to psychological stress in children, these findings suggest an opportunity to improve prehospital pain management, particularly for children with moderate pain. Limitations include the retrospective nature of this study and inability to determine whether EMS agency protocols include ibuprofen for analgesia in injured children.
Table 1. Demographics
Table 2. Demographics in patients receiving ibuprofen (N = 212)
Table 3. Description of first prehospital pharmacological analgesic treatment by various pain scores in all patients (N = 30659) a Any route
Table 1. Demographics
Table 2. Demographics in patients receiving ibuprofen (N = 212)
Table 3. Description of first prehospital pharmacological analgesic treatment by various pain scores in all patients (N = 30659) a Any route

.jpg "Kathryn Kothari, MD photo")
.png) a Any route
a Any route