
Sedation Medicine
Session: Sedation Medicine
 photo")
Ivonne E. Sierra-Strum, MD (she/her/hers)
Cardiology Fellow
Children's Hospital Los Angeles
ALHAMBRA, California, United States
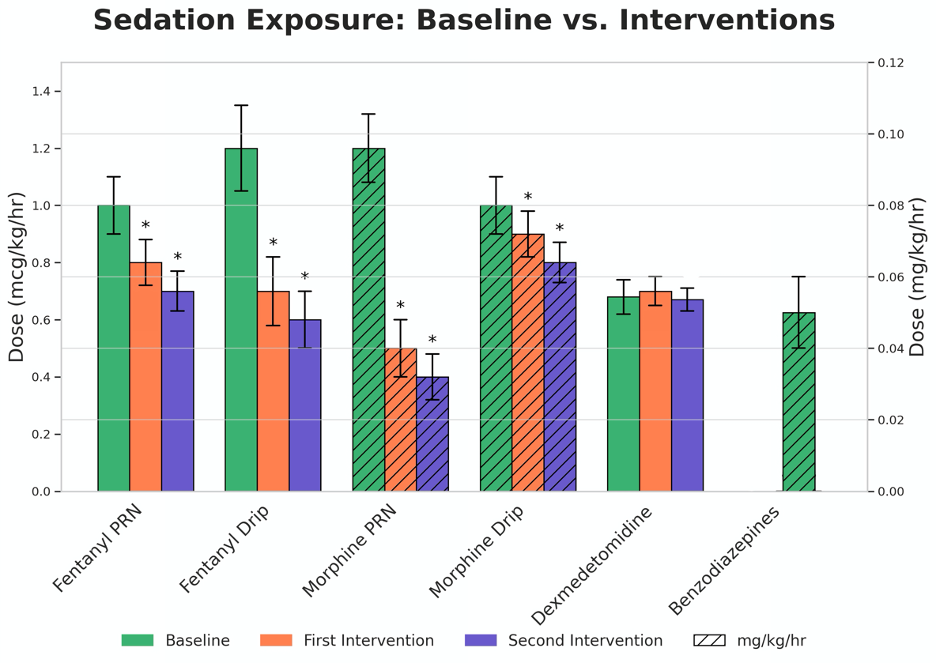 *p-Values <0.05 indicating a significant difference between Baseline and Interventions
*p-Values <0.05 indicating a significant difference between Baseline and Interventions *p-Values <0.05 indicating a significant difference between Baseline and Interventions
*p-Values <0.05 indicating a significant difference between Baseline and Interventions