
Sedation Medicine
Session: Sedation Medicine
 photo")
Edith Reyes Alvarado, MD (she/her/hers)
Assistant Professor Pediatrics
East Carolina Medical Center
Greenville, North Carolina, United States
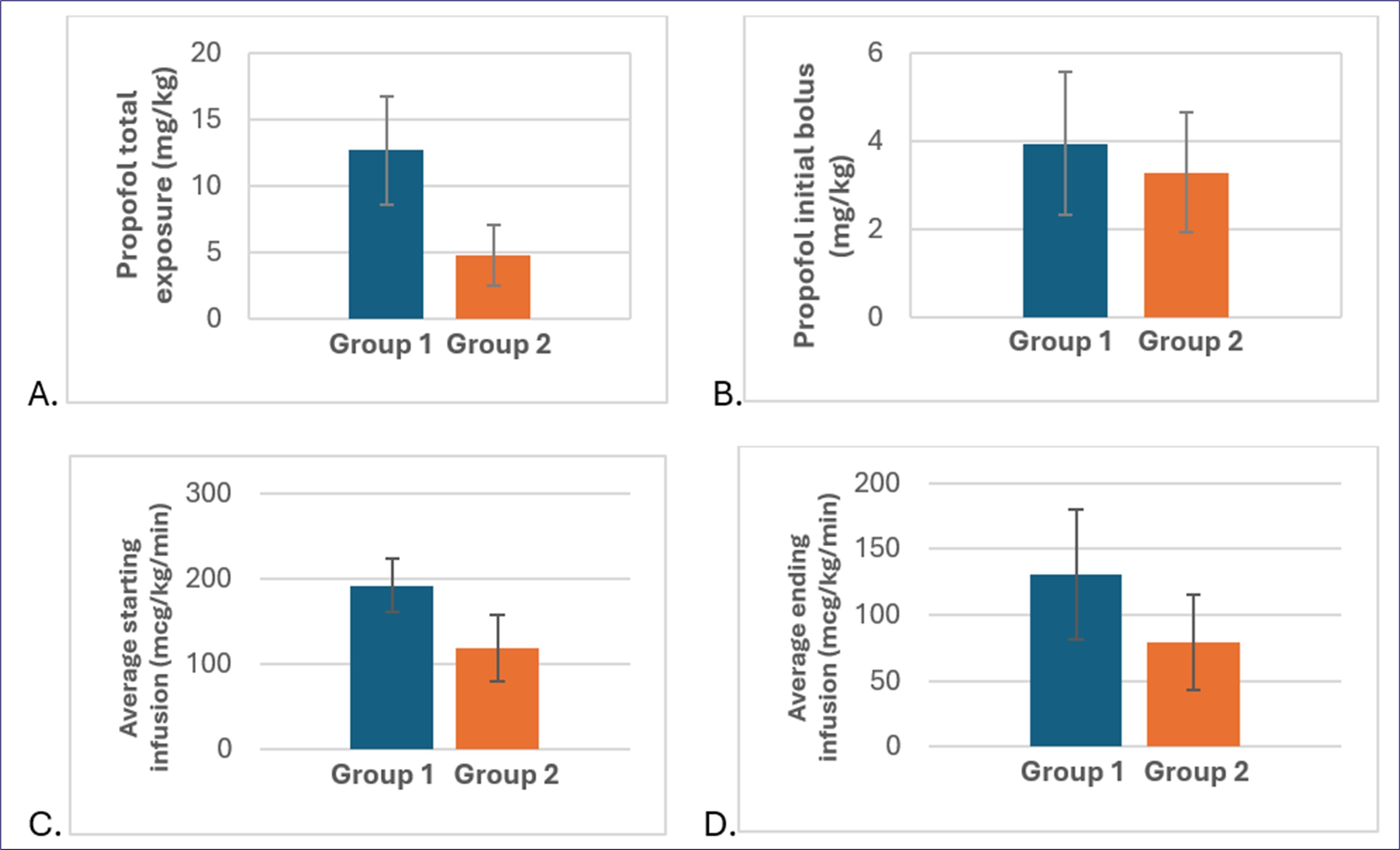 Decreases seen in: A. total dose of propofol (difference=7.85 mg/kg, p<0.001), B. bolus dose (difference=0.657 mg/kg, p=0.004), C. starting dose of continuous infusion dose (difference=72.9 mcg/kg/min, p<0.001), D. ending dose of continuous infusion (difference=51.3 mcg/kg/min, p value <0.001). Time of encounter decreased by 5 minutes (p=0.04, not shown). Intervention group 2 was pre-treated with midazolam (orange,
Decreases seen in: A. total dose of propofol (difference=7.85 mg/kg, p<0.001), B. bolus dose (difference=0.657 mg/kg, p=0.004), C. starting dose of continuous infusion dose (difference=72.9 mcg/kg/min, p<0.001), D. ending dose of continuous infusion (difference=51.3 mcg/kg/min, p value <0.001). Time of encounter decreased by 5 minutes (p=0.04, not shown). Intervention group 2 was pre-treated with midazolam (orange,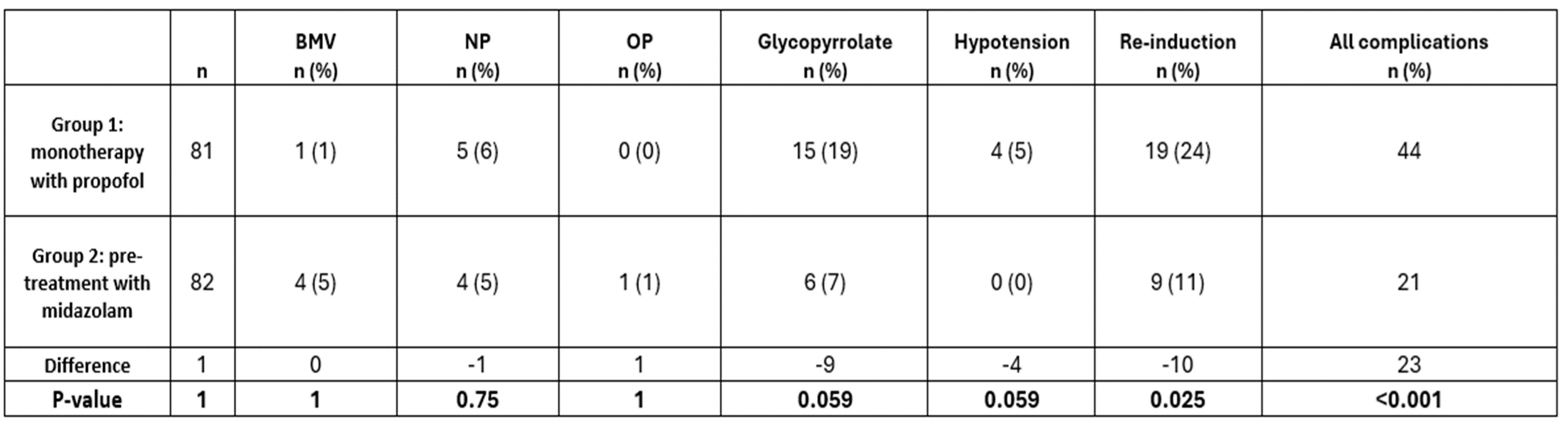 There was a significant difference between groups for all complications (last column) which was not due to any complication in particular. There were no episodes of laryngospasm, intubation, poorly perfused hypotension, or cardiopulmonary arrest in either group (not shown). Chi square test was used to compare groups. BMV =bag-mask ventilation; NP = nasopharyngeal; OP = oropharyngeal.
There was a significant difference between groups for all complications (last column) which was not due to any complication in particular. There were no episodes of laryngospasm, intubation, poorly perfused hypotension, or cardiopulmonary arrest in either group (not shown). Chi square test was used to compare groups. BMV =bag-mask ventilation; NP = nasopharyngeal; OP = oropharyngeal.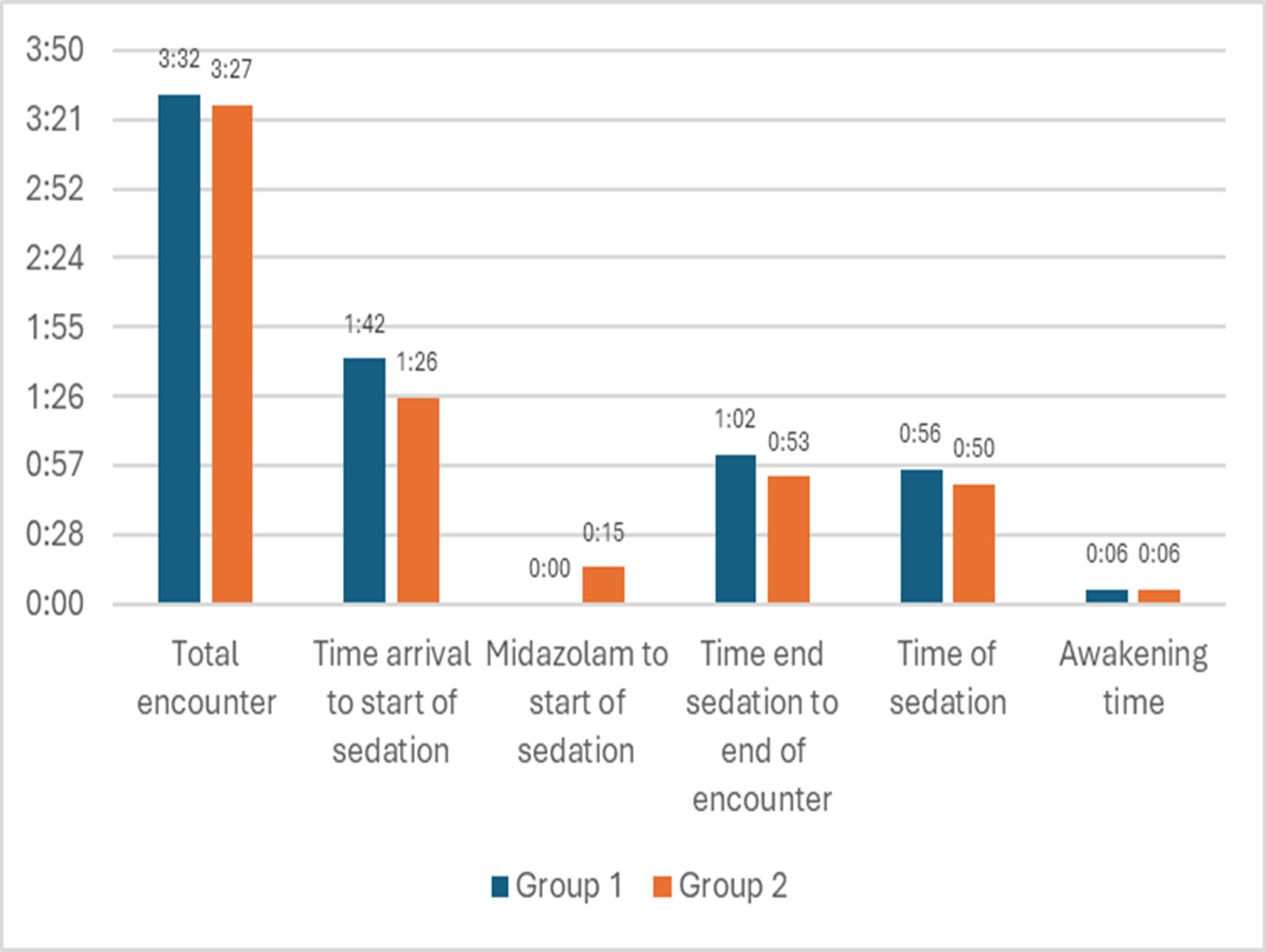 Total time of encounter (p=0.0383) and duration of sedation (p < 0.001) were decreased in group 2 (pretreatment with midazolam) compared to group 1 (control, propofol monotherapy). The following times were compared: arrival time to start of sedation, sedation time, time to awakening, and end of sedation to discharge. Time between midazolam and start of sedation applies to Group 1 only.
Total time of encounter (p=0.0383) and duration of sedation (p < 0.001) were decreased in group 2 (pretreatment with midazolam) compared to group 1 (control, propofol monotherapy). The following times were compared: arrival time to start of sedation, sedation time, time to awakening, and end of sedation to discharge. Time between midazolam and start of sedation applies to Group 1 only. 