
Children with Chronic Conditions 1
Session: Children with Chronic Conditions 1
 photo")
Erin Avondet, MD (she/her/hers)
Assistant Professor of Pediatrics
University of Utah School of Medicine
Riverton, Utah, United States
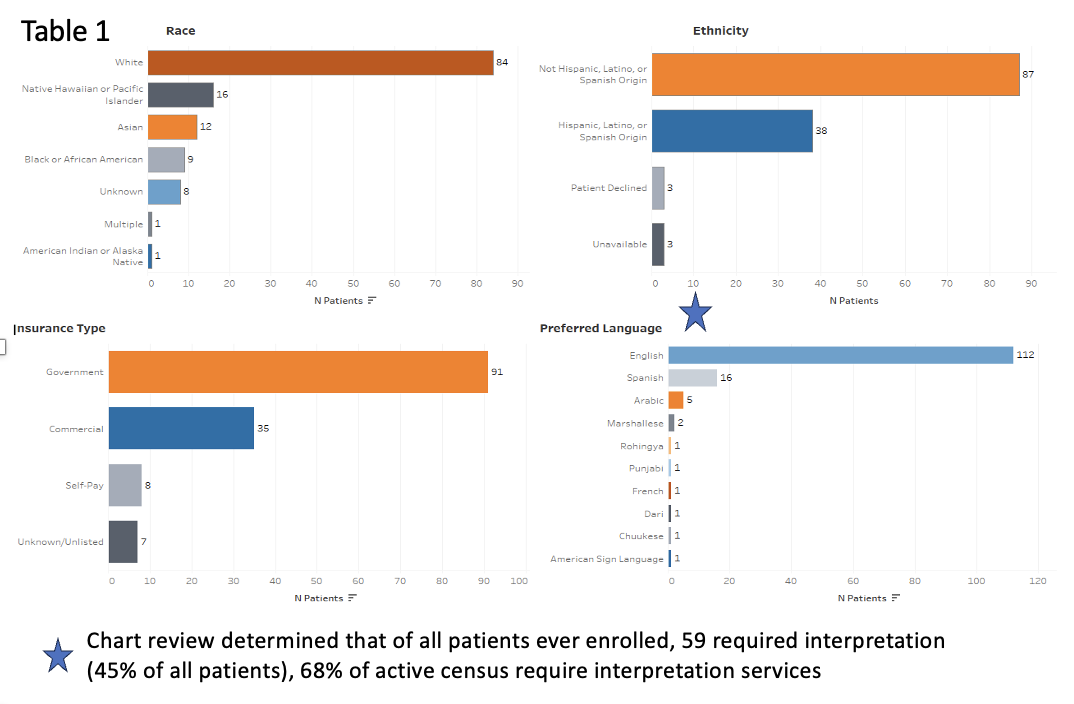 Connector Service patient demographic information
Connector Service patient demographic information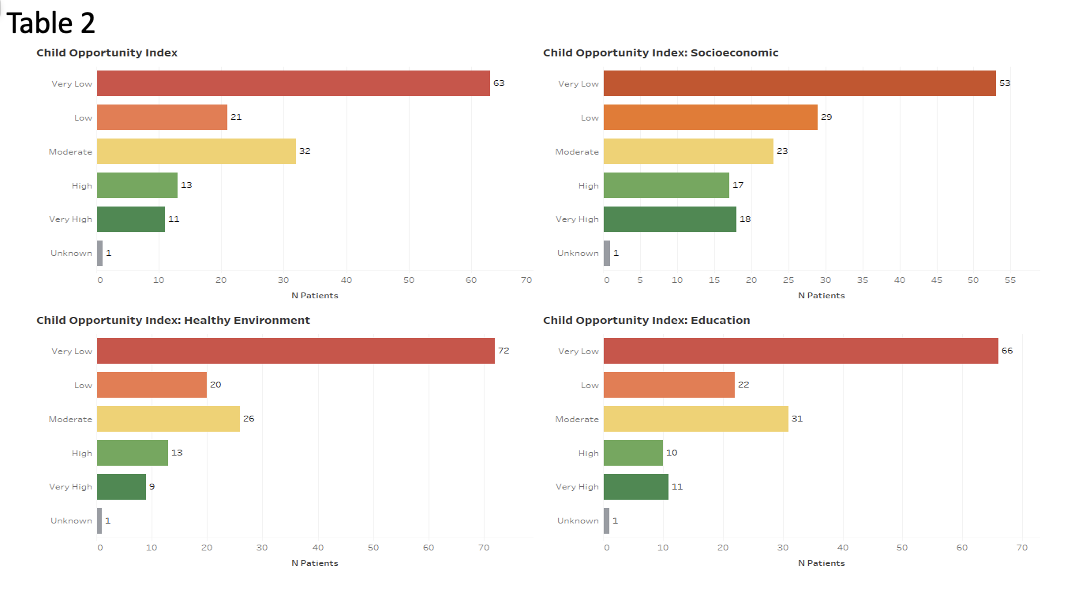 Connector Service patient COI distribution
Connector Service patient COI distribution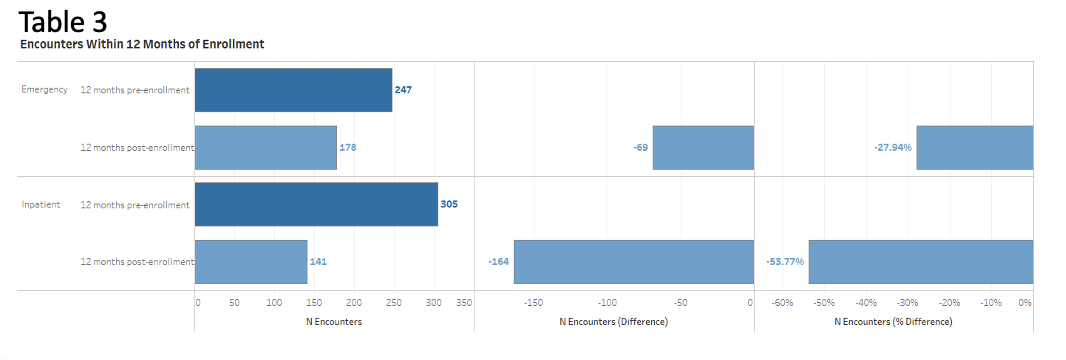 Connector Service hospital utilization data
Connector Service hospital utilization data