
Injury Prevention 1
Session: Injury Prevention 1
 photo")
Michelle Macy, MD, MS (she/her/hers)
Professor
Ann & Robert H. Lurie Children's Hospital of Chicago
Chicago, Illinois, United States
.png)
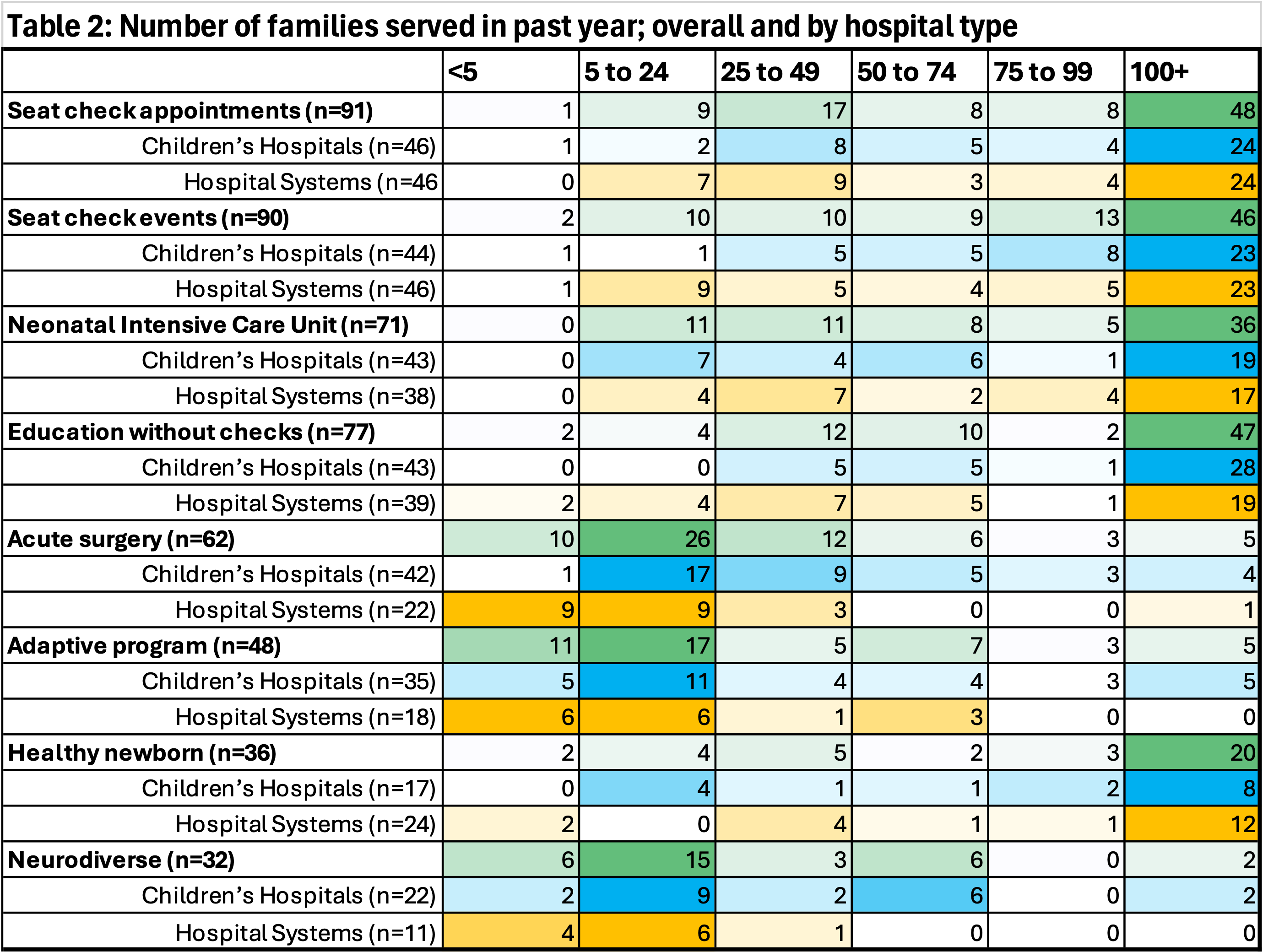 Cells are shaded from darkest to lightest within rows to indicate the largest number of hospitals to the smallest number of hospitals. Green = overall, Blue = Children's Hospitals, Yellow = Hospital System.
Cells are shaded from darkest to lightest within rows to indicate the largest number of hospitals to the smallest number of hospitals. Green = overall, Blue = Children's Hospitals, Yellow = Hospital System.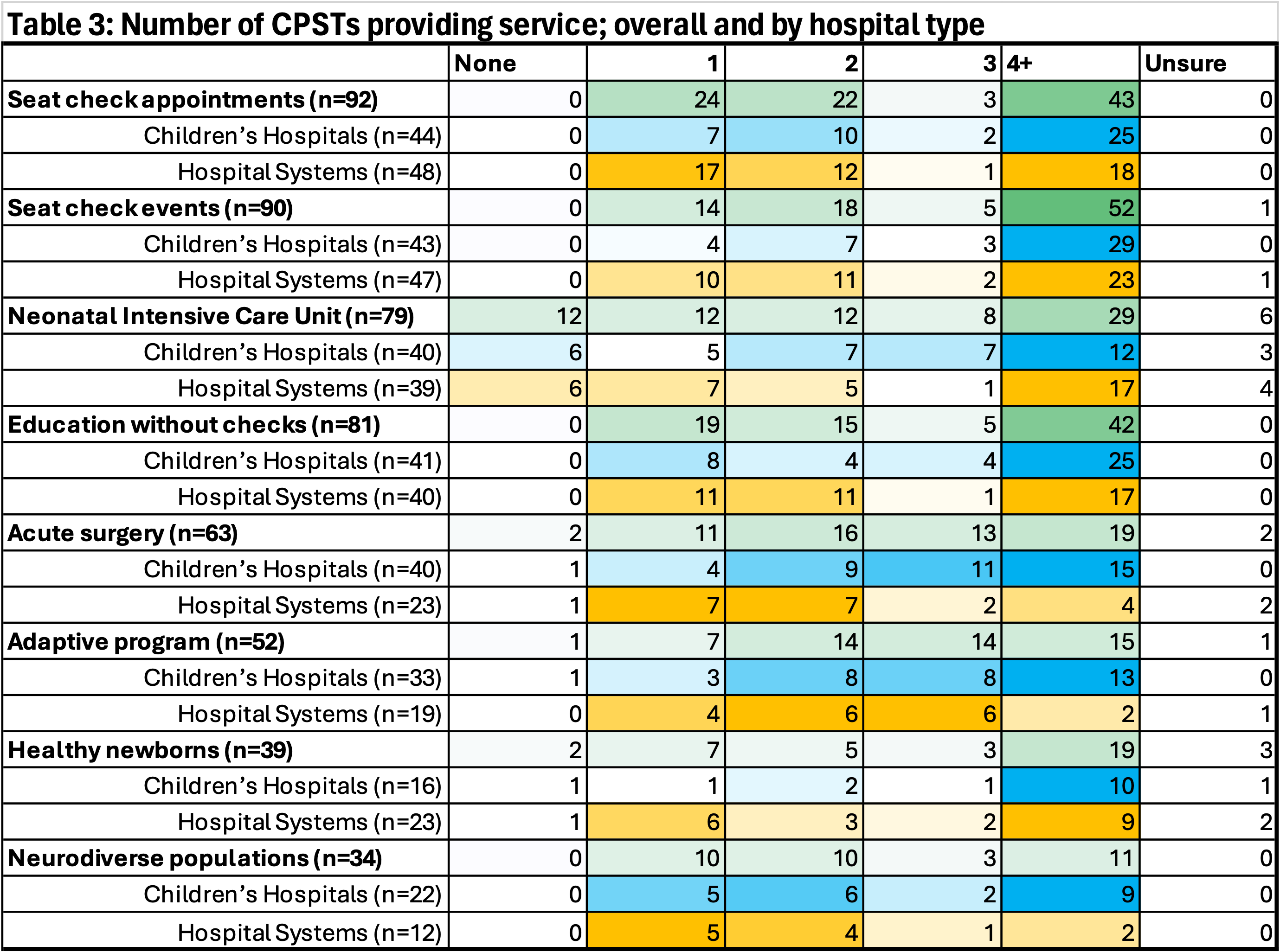 Cells are shaded from darkest to lightest within rows to indicate the largest number of hospitals to the smallest number of hospitals. Green = overall, Blue = Children's Hospitals, Yellow = Hospital System.
Cells are shaded from darkest to lightest within rows to indicate the largest number of hospitals to the smallest number of hospitals. Green = overall, Blue = Children's Hospitals, Yellow = Hospital System.