Session: Health Equity/Social Determinants of Health 5
713 - Identifying and Assessing Inequities Embedded in Clinical Guidance in Pediatric Care
Sunday, April 27, 2025
8:30am - 10:45am HST
Publication Number: 713.5380
Melissa R.. Ponce, American Academy of Pediatrics, Itasca, IL, United States; Madra Guinn-Jones, American Academy of Pediatrics, Itasca, IL, United States
Manager, Equity Science American Academy of Pediatrics Itasca, Illinois, United States
Background: Eliminating race-based medicine can appear a daunting task as bias, discrimination, and racism are deeply embedded in clinical algorithms and practice guidelines. The AAP is dedicated to a comprehensive review of its policies, guidelines, and clinical practice tools to transition to a race-conscious medicine approach. Objective: The project aim is to comprehensively review the AAP’s published clinical policies and practice guidelines to systematically analyze when bias, discrimination, and/or racism are not appropriately addressed or identified in clinical guidance. Design/Methods: A team of equity scientists with expertise in pediatric care delivery and health services research, i.e., the Rapid Revision Team (RRT), have been assembled to undertake the review of AAP policies and guide the development of a systematic process for identifying bias, discrimination, and racism in clinical guidance. The RRT identified three broad domains (explicit, insidious, and race neutral) to address problematic policies when using a race-conscious approach, policies that
•Explicitly mention race in problematic ways - e.g., using race as a biologic construct or conflating race with other social factors; •Do not explicitly mention race but rely on clinical evidence that is flawed in its consideration of race; and •Deal with clinical topics known to be plagued with inequities or with known race-based disparities but are inappropriately race neutral.
After reviewing the compendium of active CPGs/CRs, the RRT determined that the three domains included in the data abstraction form were applicable and useful in the review process and two additional domains for revision were identified. The two additional domains:
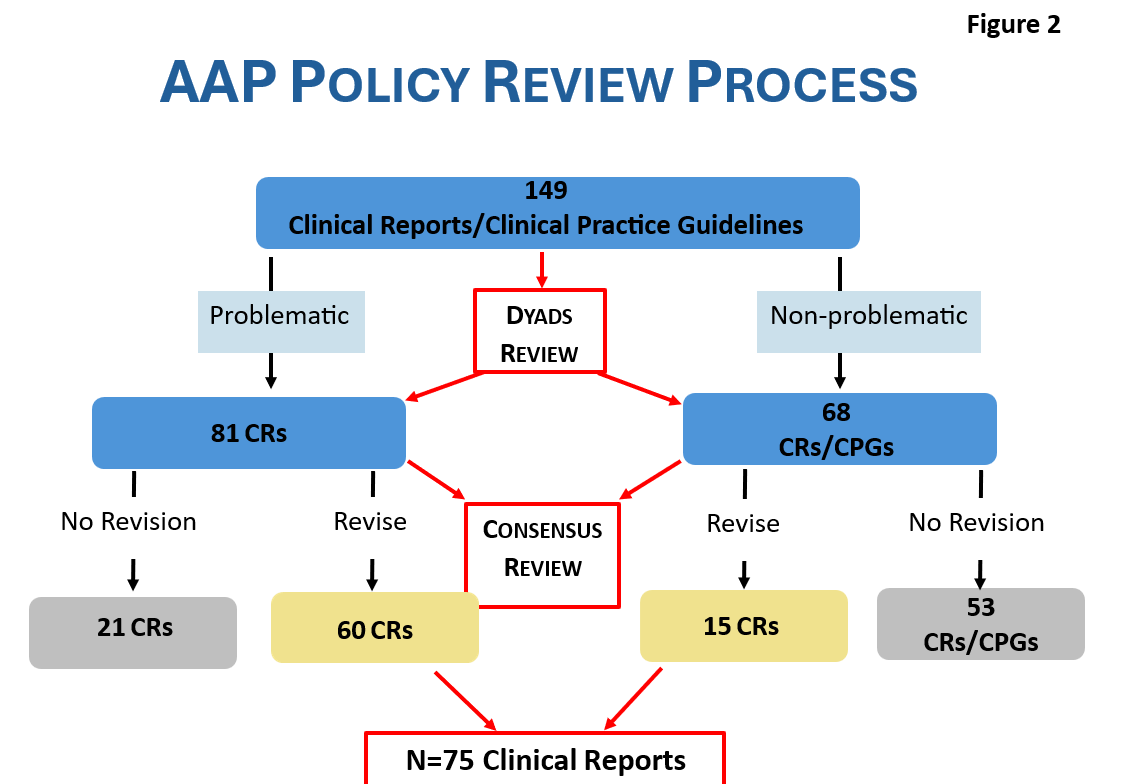
•Policies that mention outcome disparities without discussion of drivers, etiology, or proposed solutions. May perpetuate stereotypes and/or portray a biologic association between socially identified race and clinical conditions or outcomes. •Policies that include figures, tables, and/or images that are either not inclusive or present race/ethnicity in a problematic manner. Results: After the RRT reviewed all CPGs/CRs, it was determined that bias, discrimination, and/or racism was not appropriately addressed in 75 CRs that were categorized as “Needs revision” and 74 CPGs/CRs were categorized as “Does not need revision” (Figure 1).
Conclusion(s): The results demonstrate ample corrective opportunities available to transition to a race-conscious approach to develop AAP clinical guidance.

 photo")