Resident Yale New Haven Children's Hospital Shelton, Connecticut, United States
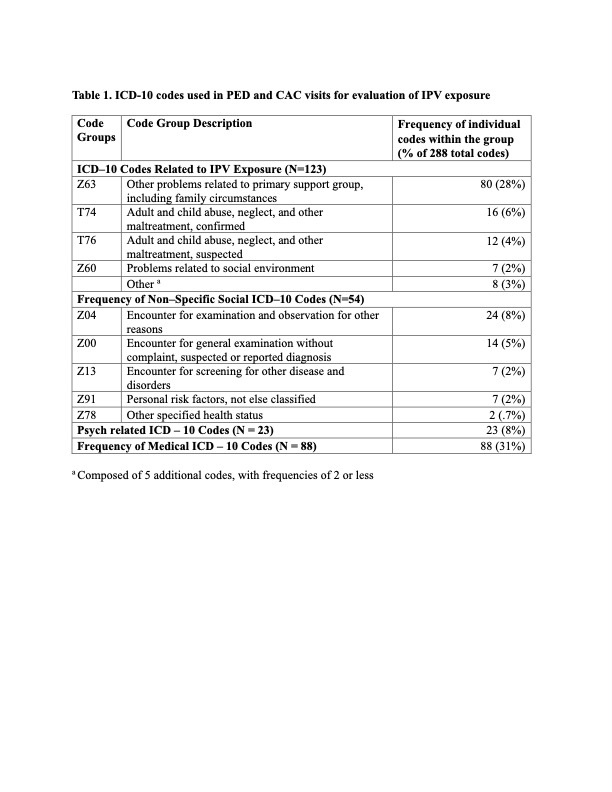
Background: Intimate partner violence (IPV) affects 1 in 3 women, often occurring in the presence of children. Such exposure at a young age has been associated with a wide array of adverse health outcomes, making early identification and intervention a public health necessity. The International Classification of Diseases, Tenth Revision (ICD-10) has been suggested as an effective tool for the identification and study of IPV, but its use in the pediatric population is uncharacterized. Objective: Identify common IPV-related diagnostic codes for children evaluated within a large urban healthcare system. Design/Methods: We performed a secondary analysis of two datasets of patient encounters for pediatric exposure to IPV between July 2019 and June 2022. Encounters were identified via a review of 1) cases of children reported to child protective services for exposure to IPV who received evaluation in either a pediatric emergency department (ED) or child advocacy center (CAC), and 2) encounters of IPV-related care in a pediatric ED in the same healthcare system. ICD–10 codes associated with each visit were descriptively summarized. A Chi-square test of independence was performed to examine the relationship between the site of evaluation (ED vs. CAC) and the use of IPV-related diagnostic codes. Results: A total of 118 pediatric encounters (65 in the ED, 53 in the CAC) were evaluated, yielding 288 distinct ICD–10 codes. 98 (83%) encounters were associated with IPV-related diagnostic codes, suspected abuse and/or a social concern (e.g., Z63, T74, T76, Z60) (table 1). CAC encounters were more likely to have IPV-related diagnostic codes when compared to ED evaluations (98% vs 70%, p = <.001).
Conclusion(s): While ICD-10 code groups Z63, T74, T76, and Z60 were frequently used in encounters of pediatric patients after IPV exposure, we identified significant variability in the use of these codes between the CAC and the PED, with CACs more frequently employing codes that reflect concerns about abuse or psychosocial circumstances. Furthermore, these code groups lack specificity for IPV, and it remains unknown if they could be used to systematically detect pediatric encounters in which IPV is identified. Given the potential risks to the safety of children and caregivers associated with the documentation of IPV in pediatric health records, ICD-10 codes may not constitute a robust mechanism for identifying such health visits. Novel approaches, such as natural language processing tools or large language models may offer superior capabilities for identifying this population within the pediatric domain.
ICD-10 codes used in PED and CAC visits for evaluation of IPV exposure a Composed of 5 additional codes, with frequencies of 2 or less

 a Composed of 5 additional codes, with frequencies of 2 or less
a Composed of 5 additional codes, with frequencies of 2 or less 