
Nephrology 5
Session: Nephrology 5
Rebecca Levy, BMBCh (she/her/hers)
Assistant Professor
University of Rochester School of Medicine and Dentistry
Rochester, New York, United States
.png) Visit-level time-varying data
Visit-level time-varying data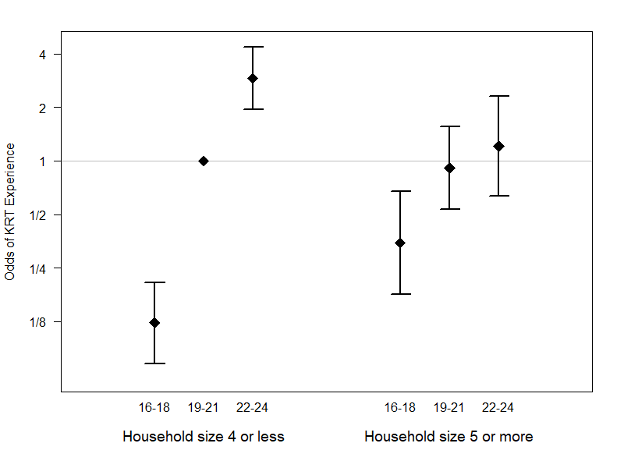 Modification of Kidney Replacement Therapy Risk by Household Size.
Modification of Kidney Replacement Therapy Risk by Household Size.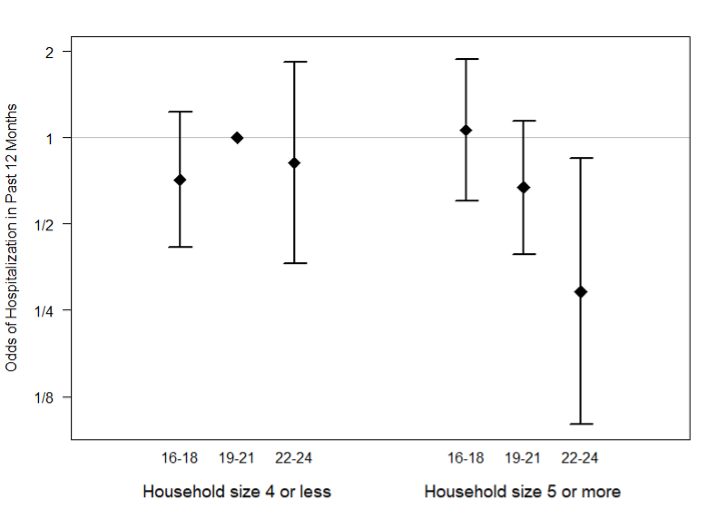 Modification of Hospitalization Risk by Household Size.
Modification of Hospitalization Risk by Household Size.