
General Pediatrics 3
Session: General Pediatrics 3

Katherine Piwnica-Worms, MD, MHS
Clinical Assistant Professor, Assistant Vice President, Pediatrics
NYU Grossman School of Medicine
New York, New York, United States
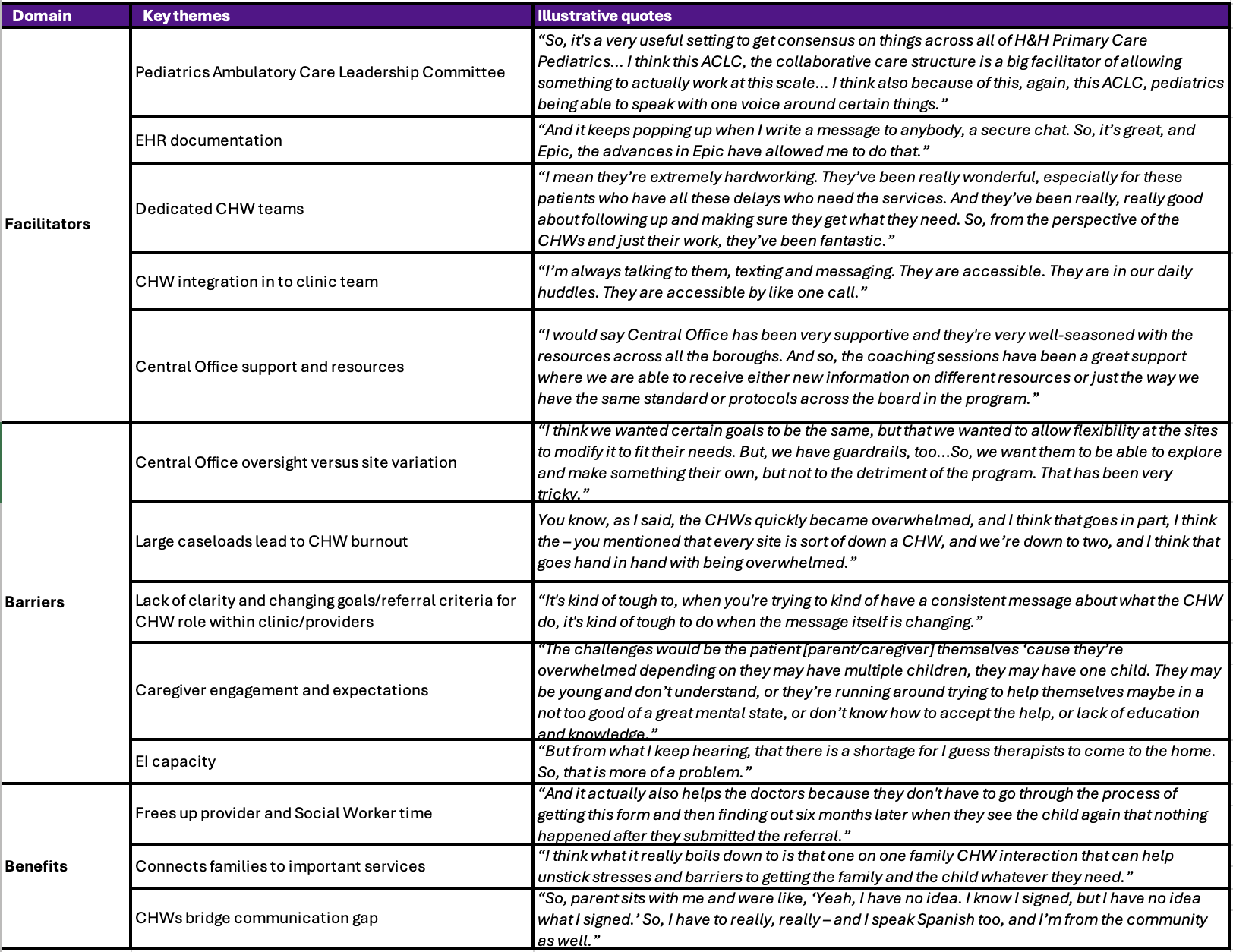 Key informants (N=41) included staff and providers at five pediatric primary care clinics, as well as members of the
Key informants (N=41) included staff and providers at five pediatric primary care clinics, as well as members of the .png) a Test statistics included paired T-test or McNemar test depending on variable structure.
a Test statistics included paired T-test or McNemar test depending on variable structure. .png) Abbreviations: EI: Early Intervention; DiD: difference-in-difference
Abbreviations: EI: Early Intervention; DiD: difference-in-difference