
Emergency Medicine 7
Session: Emergency Medicine 7
 photo")
Michael D. Johnson, MD MS (he/him/his)
Associate Professor of Pediatrics
University of Utah School of Medicine
Bountiful, Utah, United States
.png) PRAM - Pediatric Respiratory Assessment Measure; PASS - Pediatric Asthma Severity Score; AUC - area under the receiver operating characteristics curve; CI - confidence interval
PRAM - Pediatric Respiratory Assessment Measure; PASS - Pediatric Asthma Severity Score; AUC - area under the receiver operating characteristics curve; CI - confidence interval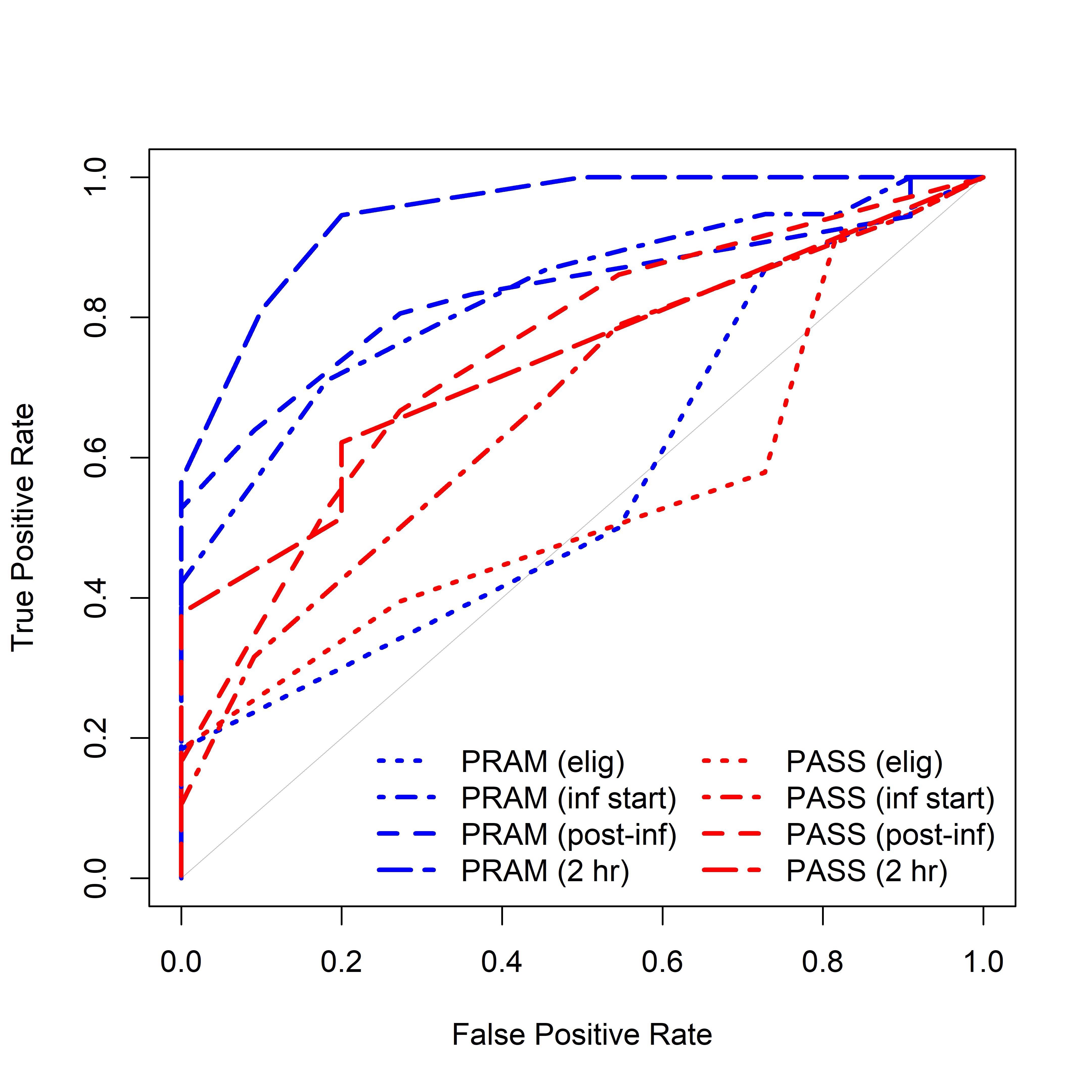 PRAM - Pediatric Respiratory Assessment Measure; PASS - Pediatric Asthma Severity Score
PRAM - Pediatric Respiratory Assessment Measure; PASS - Pediatric Asthma Severity Score