
Emergency Medicine 7
Session: Emergency Medicine 7
 photo")
Shivam Dave, MD (he/him/his)
PGY-2
UCSF Benioff Children's Hospital San Francisco
San Francisco, California, United States
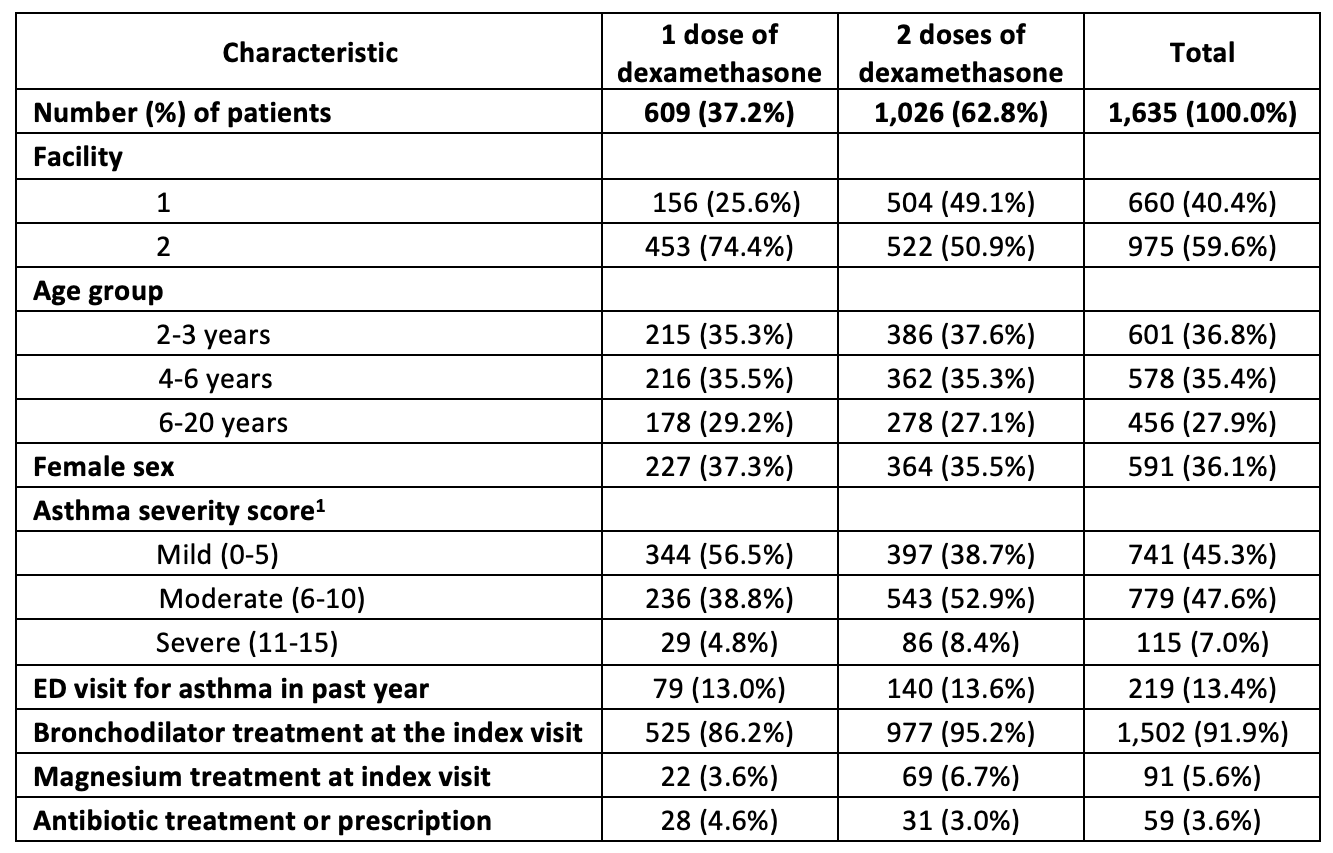 1. Based on the Modified Pediatric Asthma Severity Score, a standardized scoring system used at both facilities in this study.
1. Based on the Modified Pediatric Asthma Severity Score, a standardized scoring system used at both facilities in this study.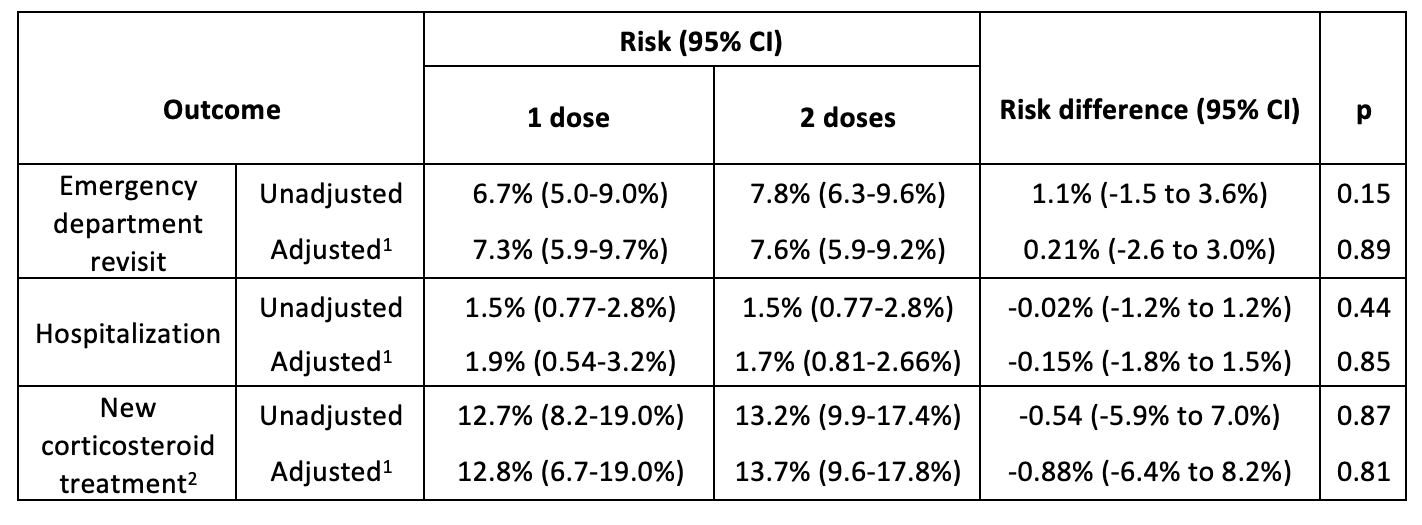 1. Adjusted risks and risks differences are from a logistic regression model weighted by the inverse probability of treatment with a second dose of dexamethasone. Propensity scores were determined by logistic regression with dexamethasone treatment (1 vs. 2 doses) as the outcome. We included the following covariates: year, facility, age, asthma severity score, prior emergency department visits for asthma, and other treatments (e.g., magnesium) at the index visit.
1. Adjusted risks and risks differences are from a logistic regression model weighted by the inverse probability of treatment with a second dose of dexamethasone. Propensity scores were determined by logistic regression with dexamethasone treatment (1 vs. 2 doses) as the outcome. We included the following covariates: year, facility, age, asthma severity score, prior emergency department visits for asthma, and other treatments (e.g., magnesium) at the index visit. 