
Endocrinology 1
Session: Endocrinology 1
Preet K. Matharu, MD (she/her/hers)
Physician Fellow
Indiana University School of Medicine
Indianapolis, Indiana, United States
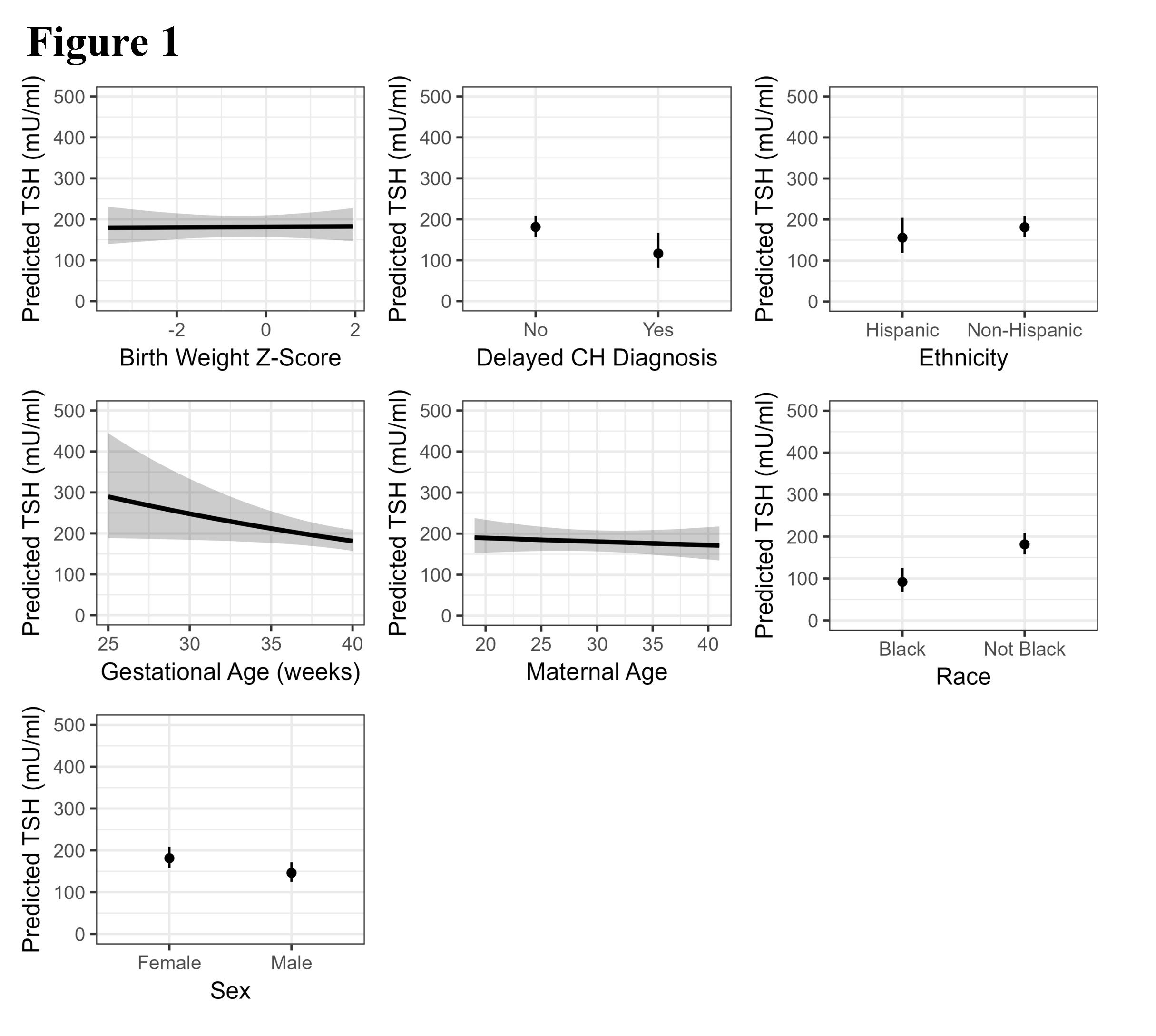 Partial effects plots for regression predicting TSH concentration. Each plot shows the predicted TSH values for a variable while all other variables in the model are held at their median (for continuous variables) or mode (for categorical variables).
Partial effects plots for regression predicting TSH concentration. Each plot shows the predicted TSH values for a variable while all other variables in the model are held at their median (for continuous variables) or mode (for categorical variables). 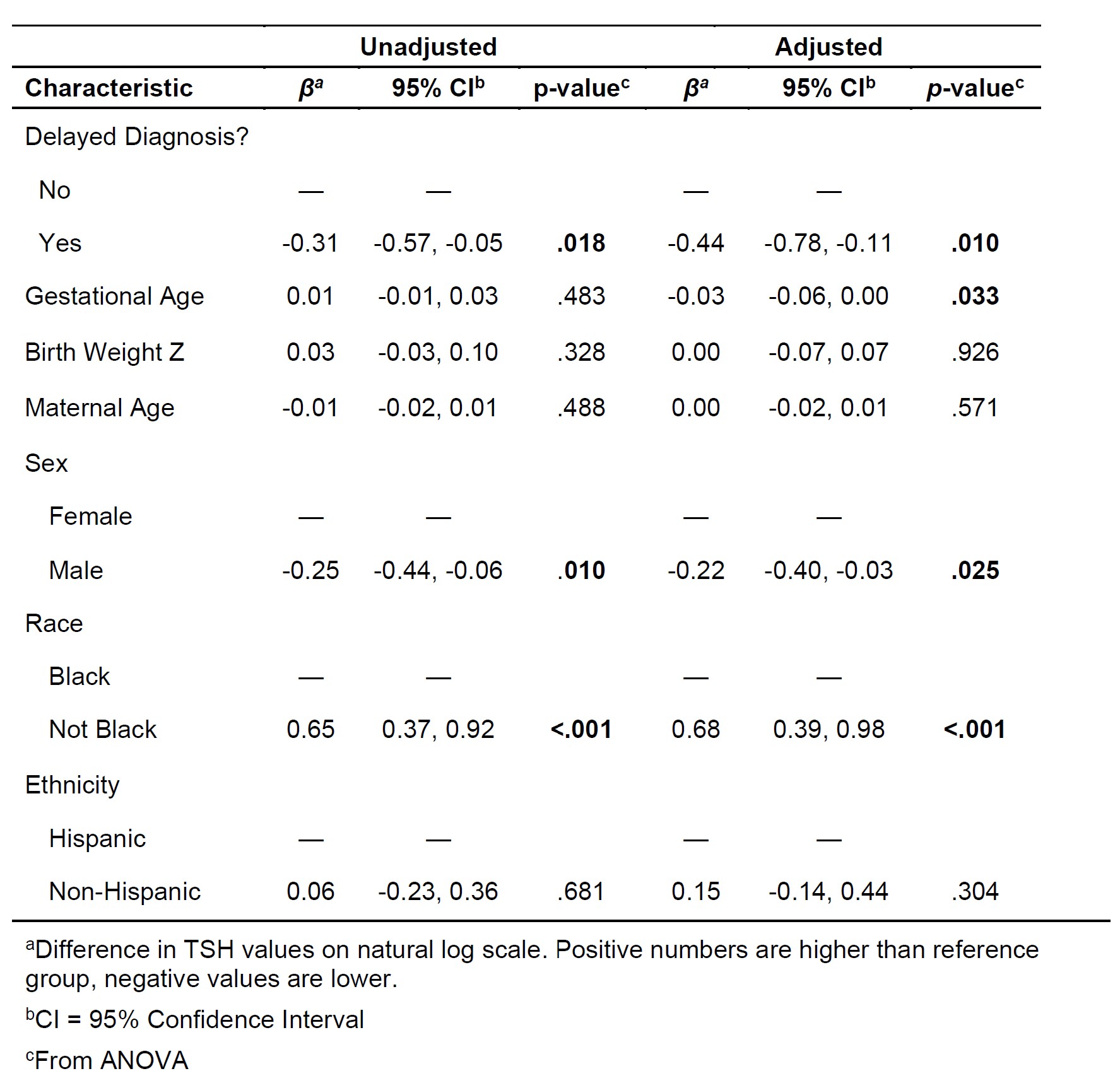 Linear regression results: variables predicting the natural logarithm of TSH concentration
Linear regression results: variables predicting the natural logarithm of TSH concentration