
Children with Chronic Conditions 1
Session: Children with Chronic Conditions 1
 photo")
Wendy Arafiles, MD, FAAP (she/her/hers)
Assistant Clinical Professor
Phoenix Children's
Phoenix, Arizona, United States
.png) Interventions implemented over the two calendar years of the initiative to improve quality and efficiency of care for CMC.
Interventions implemented over the two calendar years of the initiative to improve quality and efficiency of care for CMC.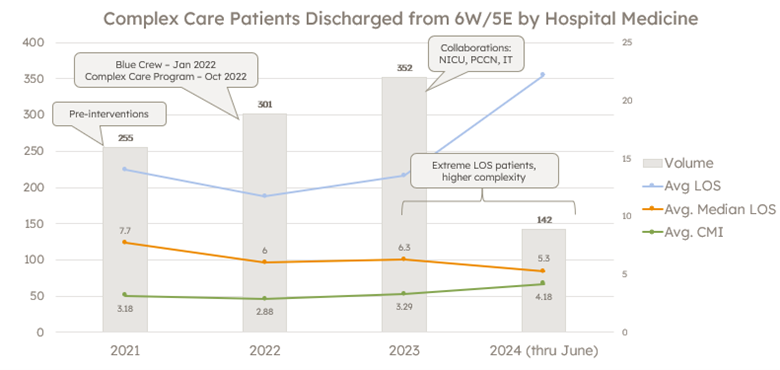 Year over year measures for volume of CMC discharged by Hospital Medicine from the inpatient unit designated for the cohort population of CMC with home invasive ventilation. LOS = length of stay; CMI = case mix index.
Year over year measures for volume of CMC discharged by Hospital Medicine from the inpatient unit designated for the cohort population of CMC with home invasive ventilation. LOS = length of stay; CMI = case mix index.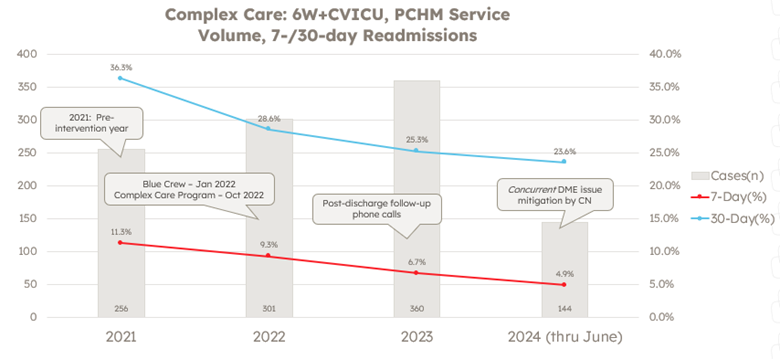 Year over year measures for 7- and 30-day unplanned readmission rates and volume of CMC discharged by Hospital Medicine from the inpatient unit designated for the cohort population of CMC with home invasive ventilation. DME = durable medical equipment; CN = care navigator
Year over year measures for 7- and 30-day unplanned readmission rates and volume of CMC discharged by Hospital Medicine from the inpatient unit designated for the cohort population of CMC with home invasive ventilation. DME = durable medical equipment; CN = care navigator