
Emergency Medicine 8
Session: Emergency Medicine 8
 photo")
Lindsey Ammann (she/her/hers)
Medical Student
University of Central Florida College of Medicine
Orlando, Florida, United States
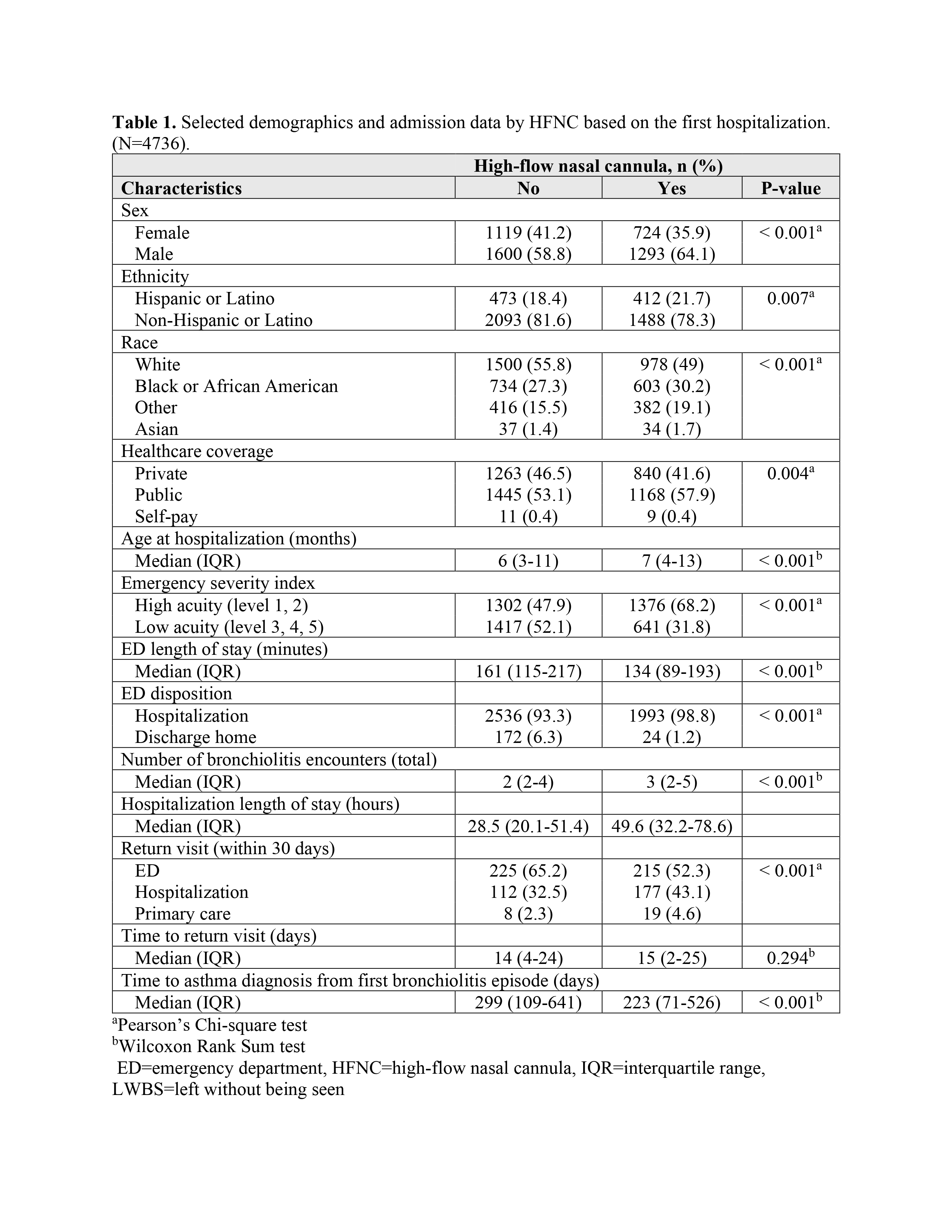 Selected demographics and admission data by HFNC based on the first hospitalization. (N=4736).
Selected demographics and admission data by HFNC based on the first hospitalization. (N=4736).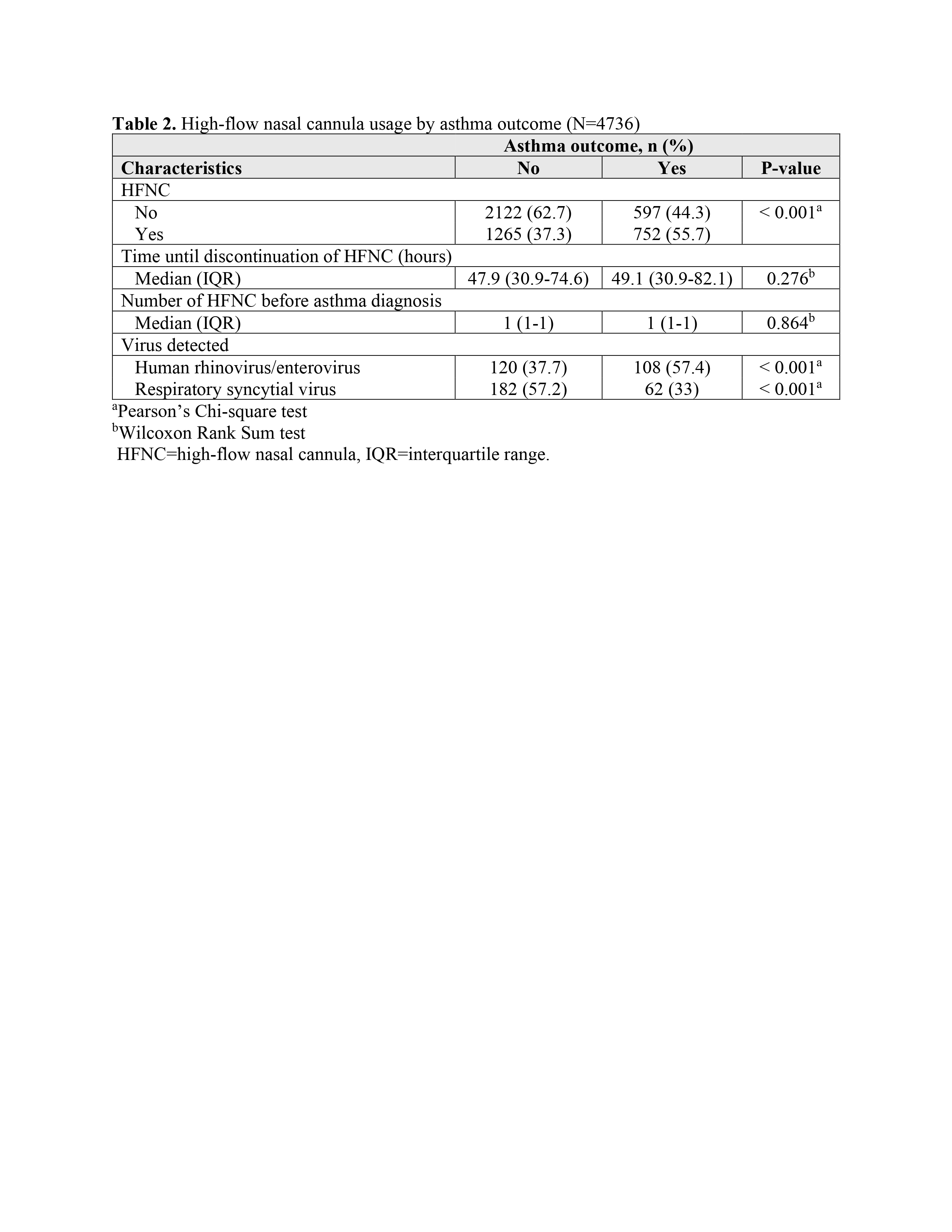 High-flow nasal cannula usage by asthma outcome (N=4736).
High-flow nasal cannula usage by asthma outcome (N=4736).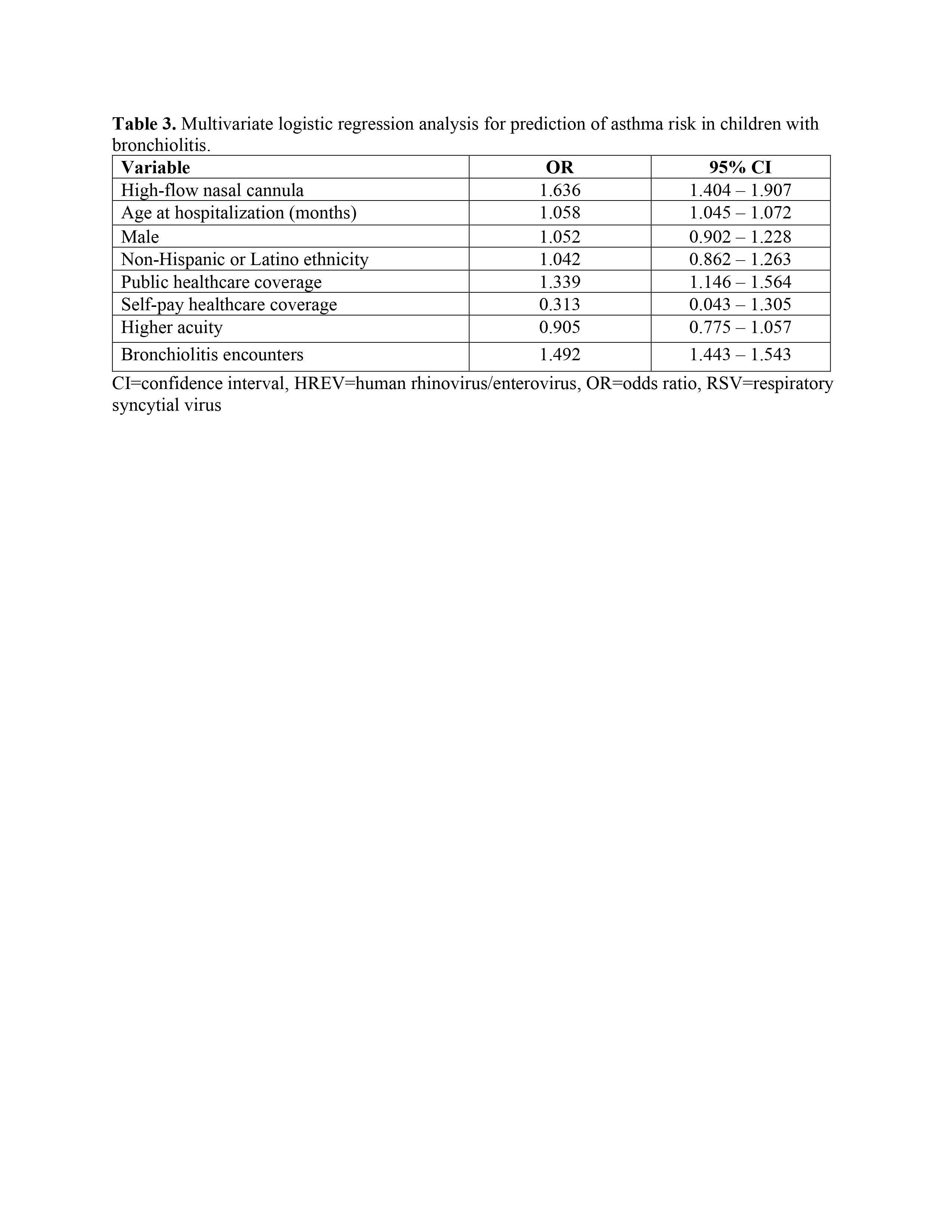 Multivariate logistic regression analysis for prediction of asthma risk in children with bronchiolitis.Selected demographics and admission data by HFNC based on the first hospitalization. (N=4736).High-flow nasal cannula usage by asthma outcome (N=4736). Multivariate logistic regression analysis for prediction of asthma risk in children with bronchiolitis.
Multivariate logistic regression analysis for prediction of asthma risk in children with bronchiolitis.Selected demographics and admission data by HFNC based on the first hospitalization. (N=4736).High-flow nasal cannula usage by asthma outcome (N=4736). Multivariate logistic regression analysis for prediction of asthma risk in children with bronchiolitis.