
Emergency Medicine 8
Session: Emergency Medicine 8
 photo")
Tara Funk Corcoran, MD (she/her/hers)
Fellow Physician
Ann & Robert H. Lurie Children's Hospital of Chicago
Chicago, Illinois, United States
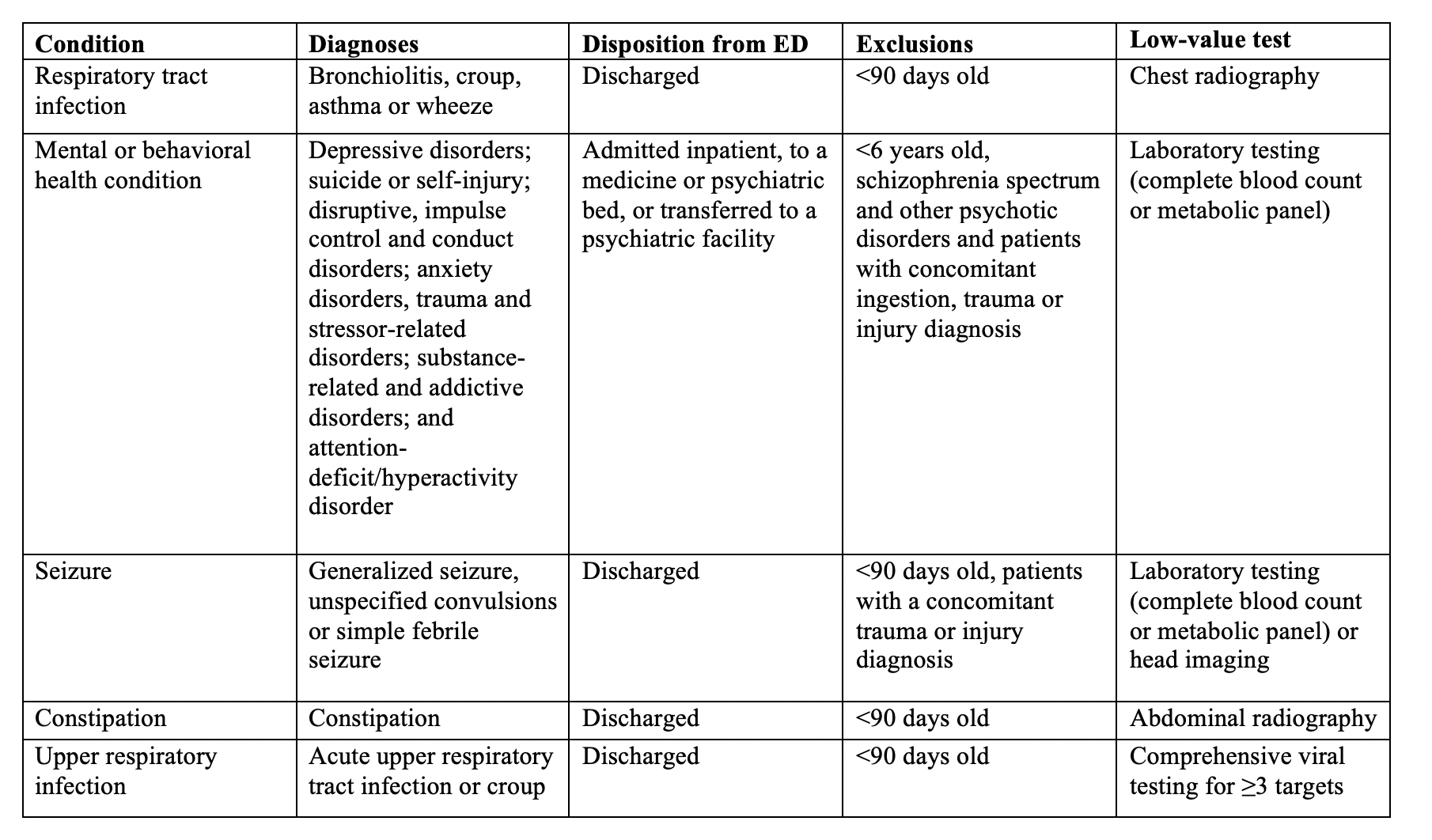 Inclusion and exclusion criteria for each studied condition
Inclusion and exclusion criteria for each studied condition.png) Low-value testing by condition, test, and hospital pediatric volume
Low-value testing by condition, test, and hospital pediatric volume.png) Longitudinal trends for low-value testing by conditionInclusion and exclusion criteria for each studied conditionLow-value testing by condition, test, and hospital pediatric volumeLongitudinal trends for low-value testing by condition
Longitudinal trends for low-value testing by conditionInclusion and exclusion criteria for each studied conditionLow-value testing by condition, test, and hospital pediatric volumeLongitudinal trends for low-value testing by condition