
Hospital Medicine 6: Clinical
Session: Hospital Medicine 6: Clinical
 photo")
Akash S. Daswaney (he/him/his)
Resident Physician, PGY-III
Charleston Area Medical Center
Charleston, West Virginia, United States
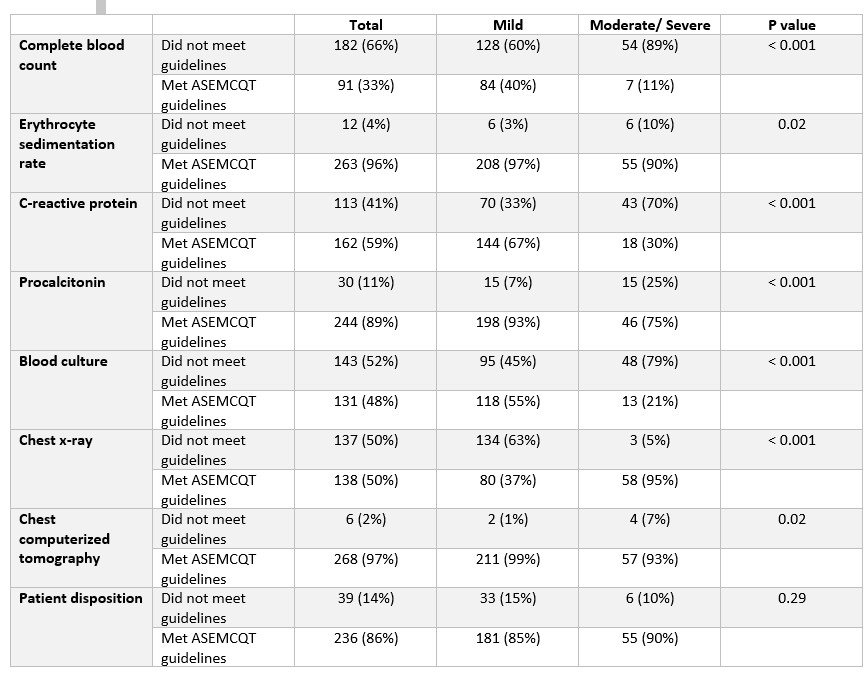 Complete blood count (CBC) and blood culture were ordered in disagreement with guidelines 66% and 52% of the time.
Complete blood count (CBC) and blood culture were ordered in disagreement with guidelines 66% and 52% of the time. 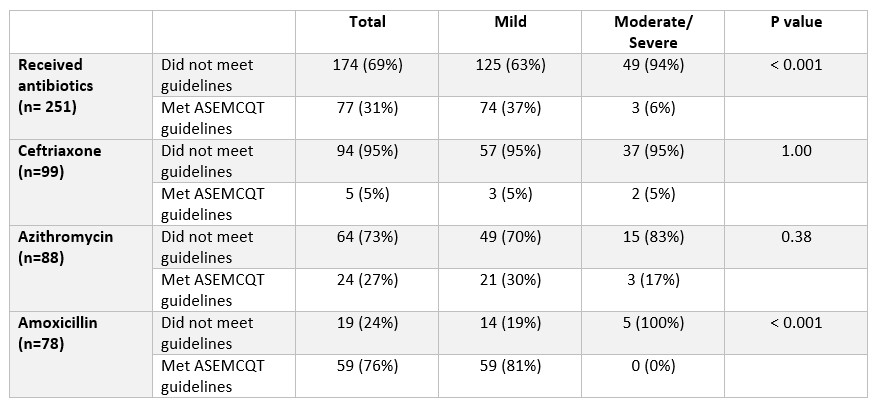 Overall, antibiotics were prescribed in disagreement with the guidelines 69% of the time, with higher non-adherence in moderate/severe cases (94%) compared to mild (63%).
Overall, antibiotics were prescribed in disagreement with the guidelines 69% of the time, with higher non-adherence in moderate/severe cases (94%) compared to mild (63%). 