
Infectious Diseases 6: Infectious diseases syndromes
Session: Infectious Diseases 6: Infectious diseases syndromes
 photo")
Natalie Chapkis, MD (she/her/hers)
Resident Physician
University of Washington School of Medicine
Seattle, Washington, United States
 Purulent discharge through the umbilicus with slight surrounding erythema demarcated by marker develops a few days into hospitalization.
Purulent discharge through the umbilicus with slight surrounding erythema demarcated by marker develops a few days into hospitalization.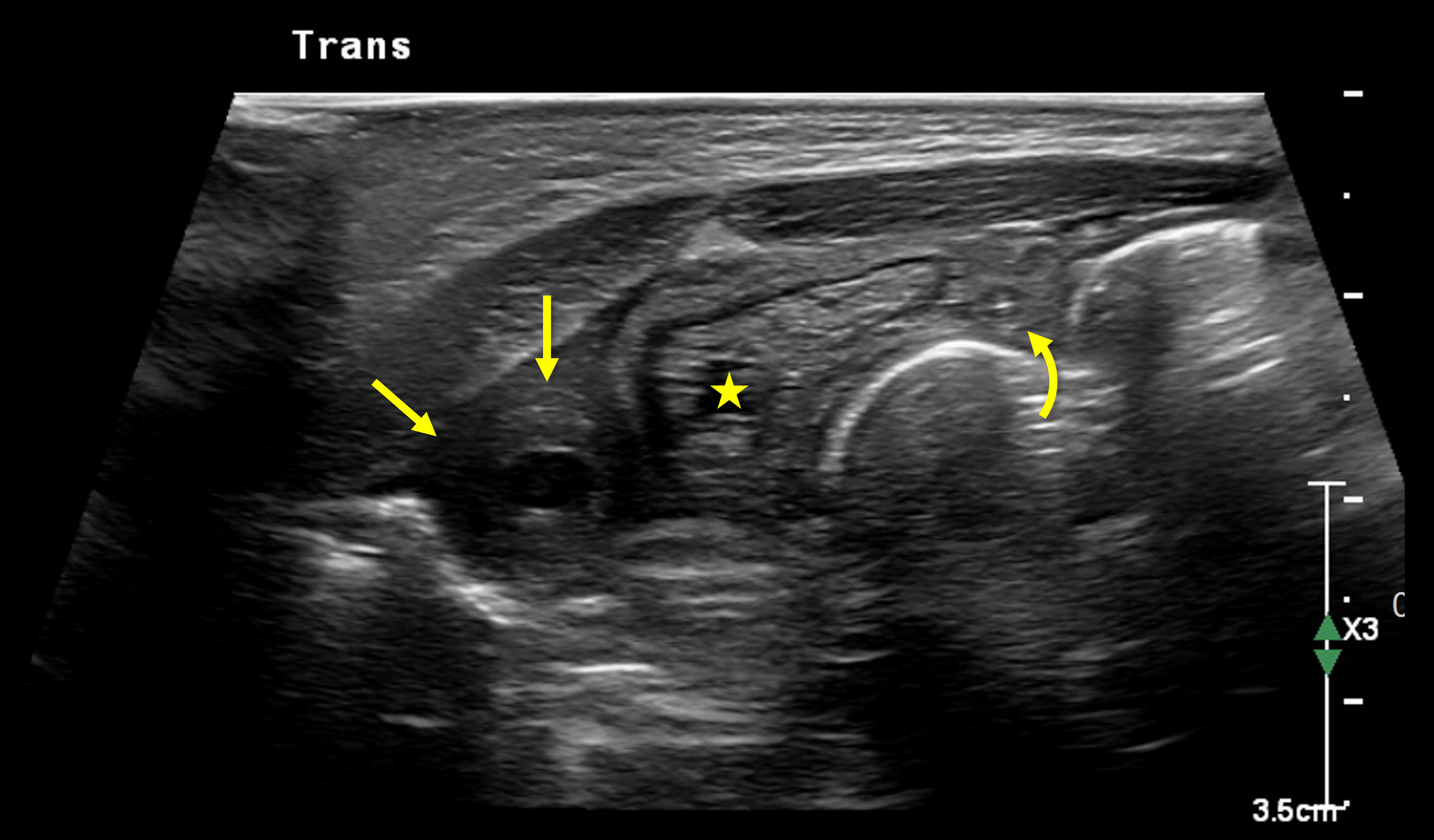 Axial ultrasound image through the midline lower abdomen at the level of the superior bladder shows asymmetry of the obliterating umbilical arteries. The right artery (straight arrows) is hypoechoic, thickened, and enlarged compared to the left (curved arrow). These paired structures course laterally to the bladder dome (star).
Axial ultrasound image through the midline lower abdomen at the level of the superior bladder shows asymmetry of the obliterating umbilical arteries. The right artery (straight arrows) is hypoechoic, thickened, and enlarged compared to the left (curved arrow). These paired structures course laterally to the bladder dome (star).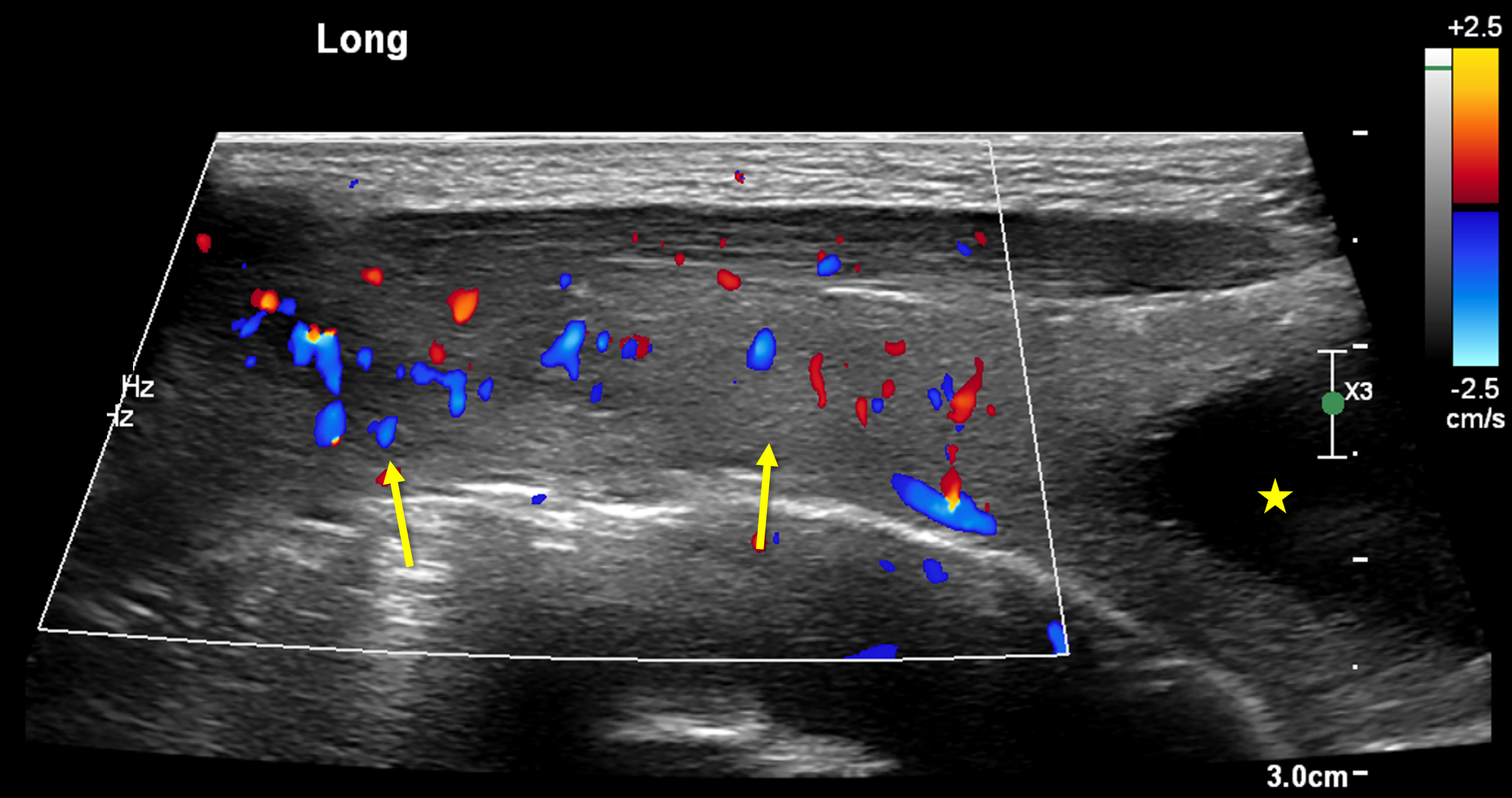 Longitudinal Doppler ultrasound image of the right para-midline abdomen, focused on the right umbilical artery (arrows). There is increased Doppler signal (red and blue color) on the right compared to the left (not shown), consistent with abnormal inflammation of the thrombosed obliterating umbilical artery.
Longitudinal Doppler ultrasound image of the right para-midline abdomen, focused on the right umbilical artery (arrows). There is increased Doppler signal (red and blue color) on the right compared to the left (not shown), consistent with abnormal inflammation of the thrombosed obliterating umbilical artery.