103 - Shifting Epidemiology of Mycoplasma pneumoniae and Relative Burden of Community Acquired Pneumonia (CAP) ED Visits. Metropolitan Atlanta, GA. 1/4/2016-10/27/2024.
Sunday, April 27, 2025
8:30am - 10:45am HST
Publication Number: 103.6989
Sujit Sharma, Children's Healthcare of Atlanta, Roswell, GA, United States; carlos delgado, CHOA, Suwanee, GA, United States
Vice Section Director Division of Emergency Medicine Children's Healthcare of Atlanta Roswell, Georgia, United States
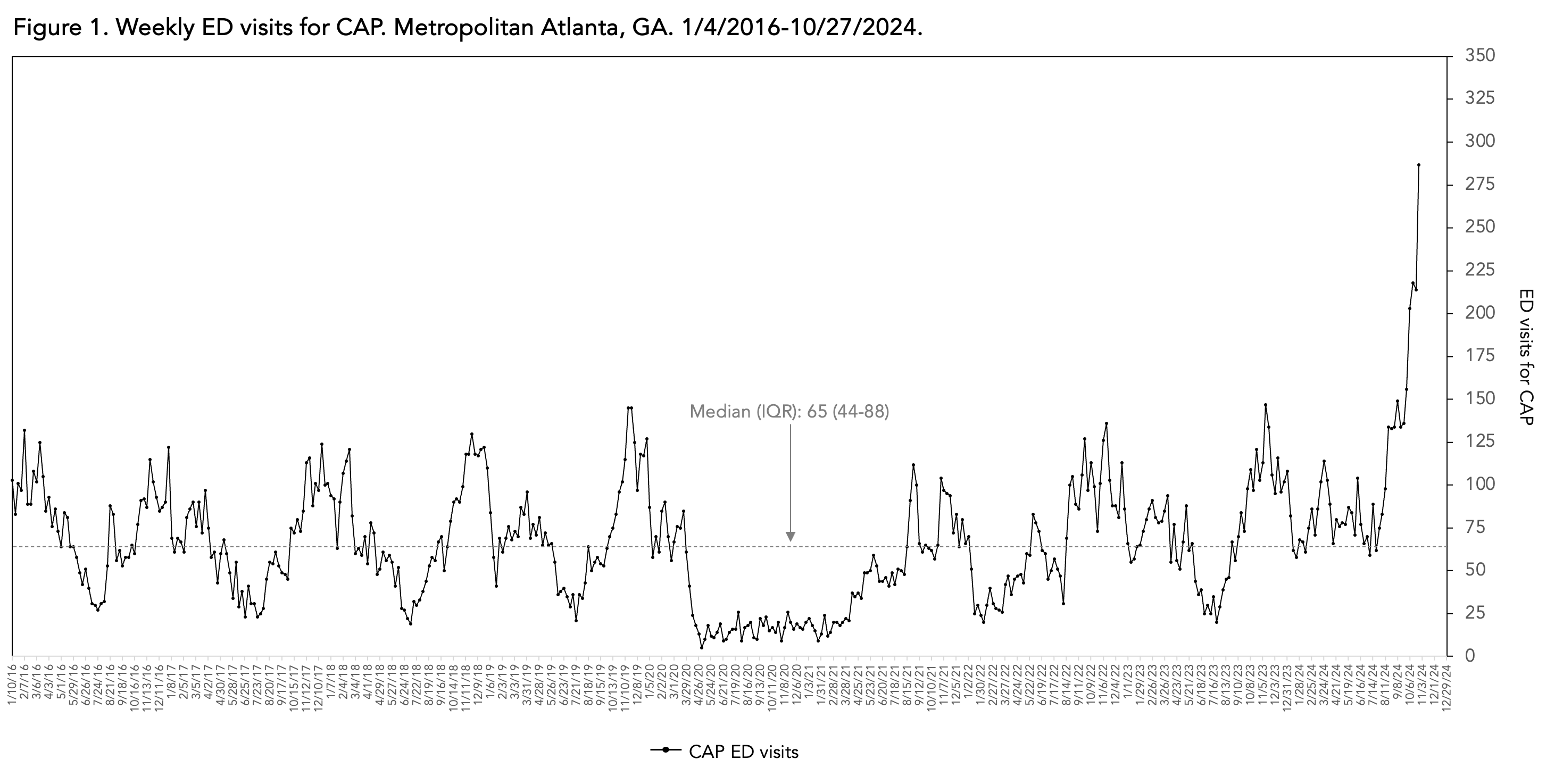
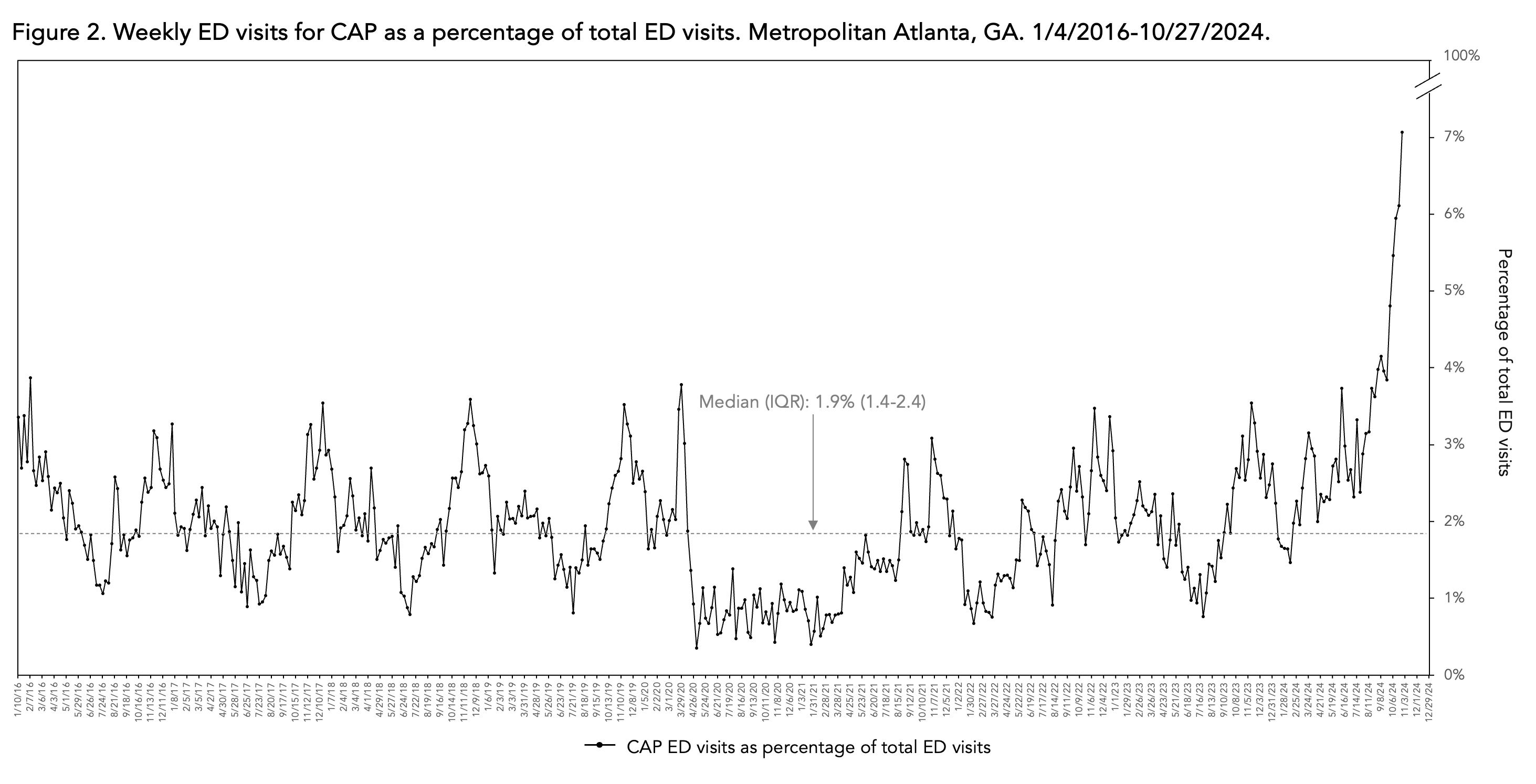
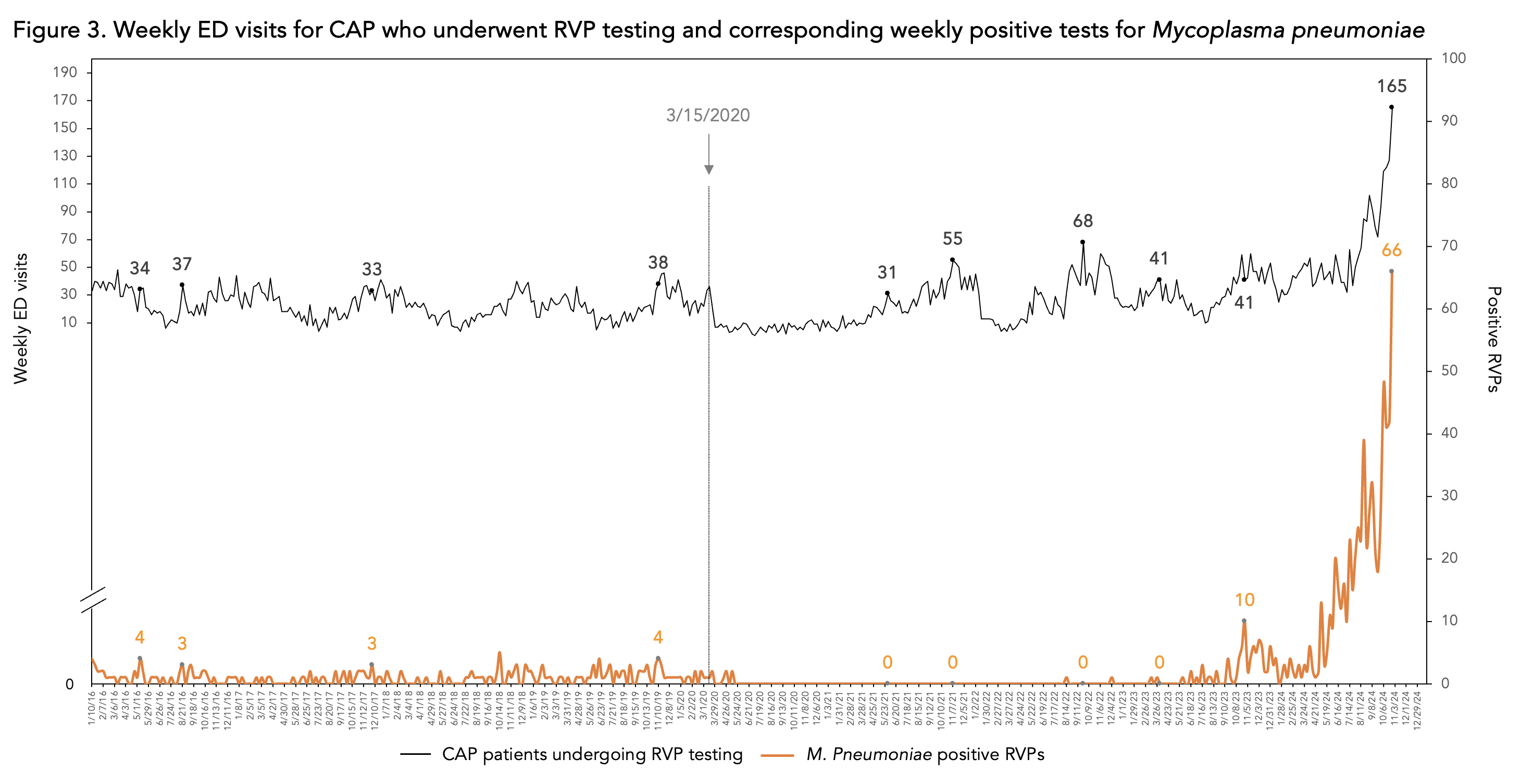
Background: Community acquired pneumonia (CAP) is a frequent cause of pediatric emergency department (ED) visits and hospitalizations. Prior to the pandemic caused by SARS-CoV-2, Mycoplasma pneumoniae (M. pneu) caused approximately 5% of CAP in children (less than 18 years of age). Objective: Characterize the dynamic and evolving fluctuation of CAP visits associated with M. pneu circulation in 2024, and in comparison to pre- and post-SARS-CoV-2 pandemic patterns in a large pediatric quaternary care system. Design/Methods: We retrospectively reviewed electronic medical records to identify weekly (Mon-Sun) total ED visits and ED visits associated with primary or secondary ICD-10 diagnosis codes encompassing pneumonia diagnoses, which we herein collectively refer to as CAP. We further identified those with CAP who underwent multiplex nasopharyngeal respiratory viral panel (RVP) polymerase chain reaction testing and were positive for M. pneu. We have quantified the volume of total ED visits, ED visits for CAP, RVP testing/results among patients with CAP, and provided a descriptive analysis of longitudinal trends in patient volumes and positive M. pneu RVPs. Results: During the 460-week study period (1/4/2016-10/27/2024), there were 1,506,973 ED visits, and 30,789 ED visits (2%) for CAP. The median (IQR) weekly visit rate for CAP was 65 (42-88). (Figure 1) As a percentage of weekly ED visits, the median (IQR) for CAP was 1.9% (1.4%-2.4%) (Figure 2). During the pre-pandemic period (1/4/2016-3/15/2020), M. pneu positive PCRs among CAP patients who underwent RVP testing was low, but frequently present. During the 185-week post-pandemic period between 3/16/2020-10/1/2023, M. pneu positive PCRs among CAP patients who had RVP testing became negligible, despite the volume of pneumonia visits returning to pre-pandemic levels in late 2021. Beginning with the back-to-school period (early August) in 2024, the steady increase in CAP patients undergoing RVP testing was associated with a steady and substantial increase in the number of M. pneu positive tests. (Figure 3)
Conclusion(s): Pre-SARS-CoV-2 pandemic patterns of CAP in metropolitan Atlanta demonstrate that M. pneu was an infrequent but persistent cause of CAP. However, the resurgence of M. pneu during the post back-to-school period in 2024 has been associated with unparalleled (and ongoing) levels of off-season ED visits for CAP. Our data suggest that M. pneu reemergence is coinciding with (and benefitting from) waning population-level immunological memory resulting from non-pharmacological interventions enacted during the early phases of the SARS-CoV-2 pandemic.
Figure 1. Weekly ED visits for CAP. Metropolitan Atlanta, GA. 1/4/2016-10/27/2024.
Weekly ED visits for CAP as a percentage of total ED visits. Metropolitan Atlanta, GA. 1/4/2016-10/27/2024.
Weekly ED visits for CAP who underwent RVP testing and corresponding weekly positive tests for Mycoplasma pneumoniae

.jpg "Sujit Sharma, MD photo")