
Child Abuse & Neglect 1
Session: Child Abuse & Neglect 1
Henry T. Puls, MD
Professor of Pediatrics
Children's Mercy Kansas City
Kansas City, Missouri, United States
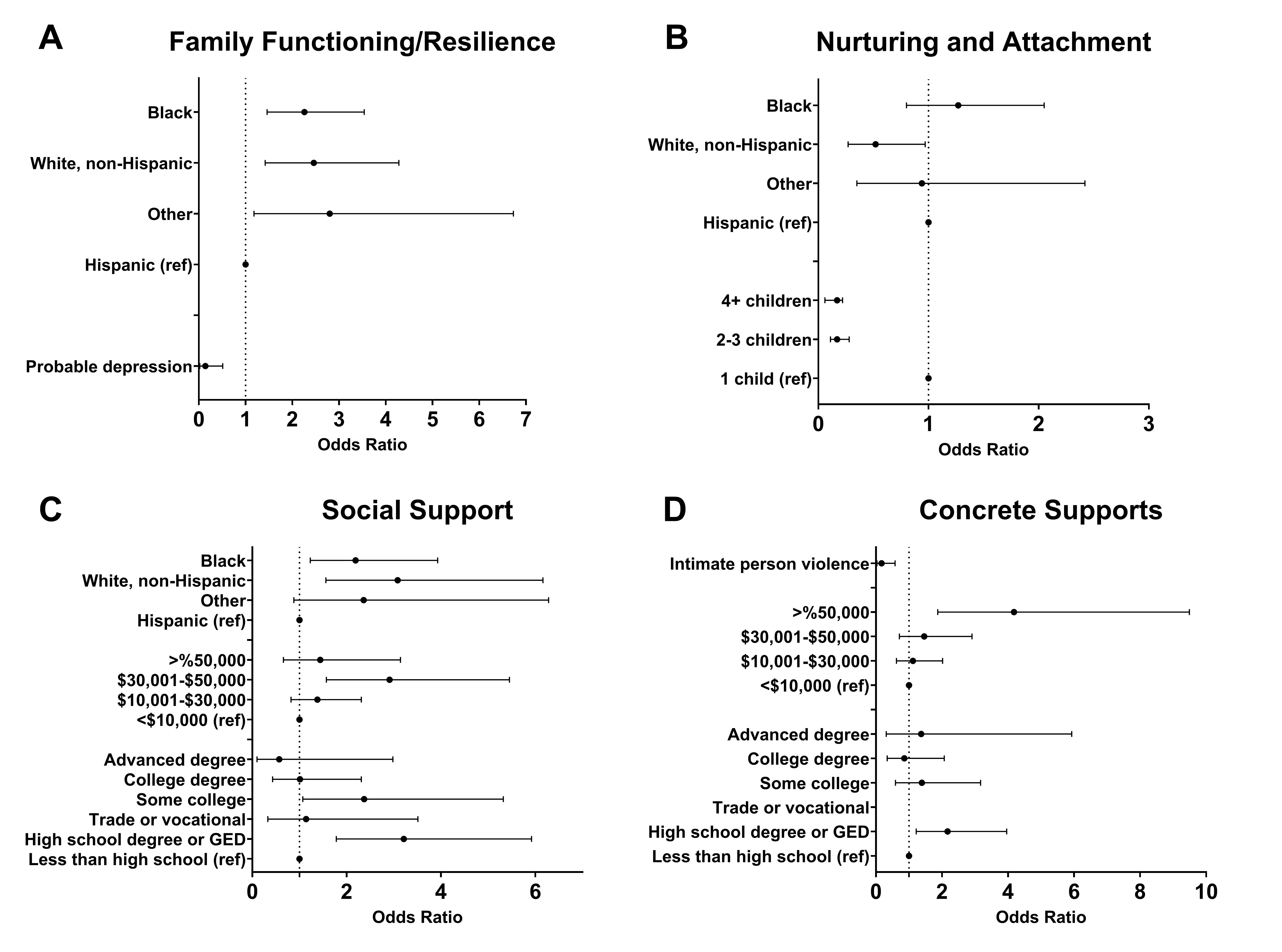 Adjusted odds of optimal PF subscale scores, (A) Family Functioning/Resilience, (B) Nurturing and Attachment, (C) Social Support, (D) Concrete Supports. All maternal demographics and risk factors with near significance in bivariate analysis (i.e., p< 0.1) were included in the initial multivariable logistic regression models. Race and ethnicity was of specific interest as a primary exposure and was initially included in all 4 subscale regression models. Non-significant covariates were removed using backwards elimination. Adjusted odds of optimal PF subscale scores, (A) Family Functioning/Resilience, (B) Nurturing and Attachment, (C) Social Support, (D) Concrete Supports. All maternal demographics and risk factors with near significance in bivariate analysis (i.e., p< 0.1) were included in the initial multivariable logistic regression models. Race and ethnicity was of specific interest as a primary exposure and was initially included in all 4 subscale regression models. Non-significant covariates were removed using backwards elimination.
Adjusted odds of optimal PF subscale scores, (A) Family Functioning/Resilience, (B) Nurturing and Attachment, (C) Social Support, (D) Concrete Supports. All maternal demographics and risk factors with near significance in bivariate analysis (i.e., p< 0.1) were included in the initial multivariable logistic regression models. Race and ethnicity was of specific interest as a primary exposure and was initially included in all 4 subscale regression models. Non-significant covariates were removed using backwards elimination. Adjusted odds of optimal PF subscale scores, (A) Family Functioning/Resilience, (B) Nurturing and Attachment, (C) Social Support, (D) Concrete Supports. All maternal demographics and risk factors with near significance in bivariate analysis (i.e., p< 0.1) were included in the initial multivariable logistic regression models. Race and ethnicity was of specific interest as a primary exposure and was initially included in all 4 subscale regression models. Non-significant covariates were removed using backwards elimination. 