
Child Abuse & Neglect 1
Session: Child Abuse & Neglect 1
 photo")
Michael D. Fishman, MD (he/him/his)
Pediatric Emergency Medicine Fellow
Boston Children's Hospital
Boston Children's Hospital, Boston Medical Center
Boston, Massachusetts, United States
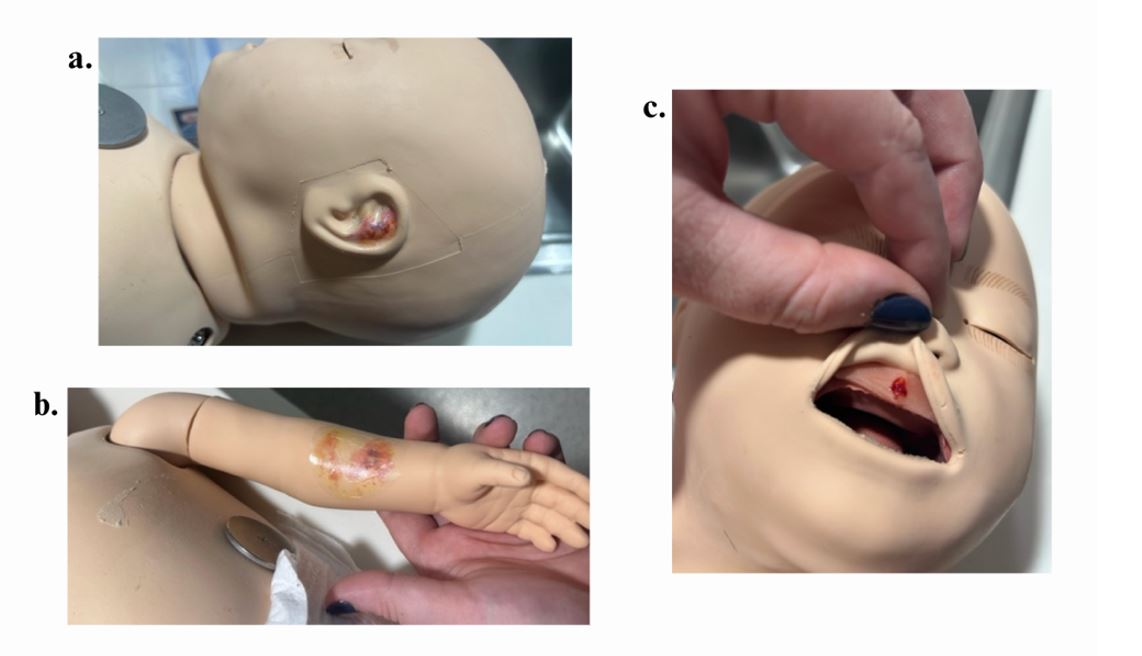 Simulation manikin moulage: a. ear bruise; b. forearm bruise; and c. frenula injury.
Simulation manikin moulage: a. ear bruise; b. forearm bruise; and c. frenula injury.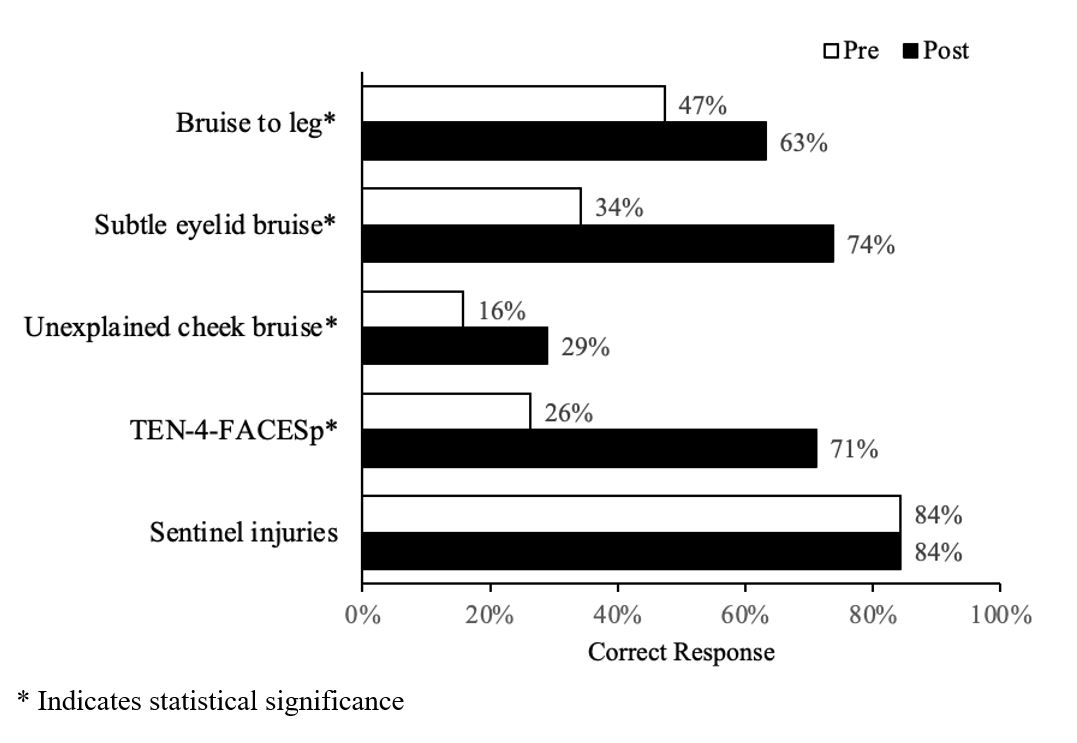 Percentage of participants who correctly answered knowledge-based questions on linked pre- and post-survey.
Percentage of participants who correctly answered knowledge-based questions on linked pre- and post-survey.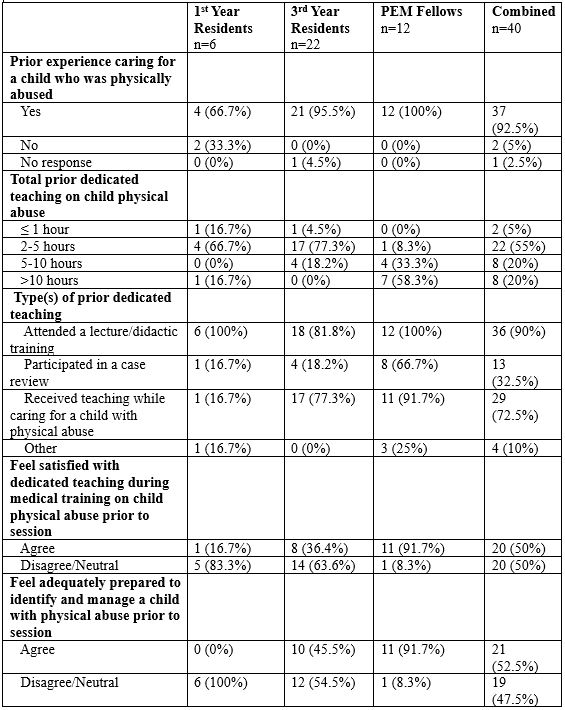 Participant characteristics.
Participant characteristics.