
Breastfeeding/Human Milk 2
Session: Breastfeeding/Human Milk 2

Yohanna Tesfaye, MD
Resident
Baylor College of Medicine
Houston, Texas, United States
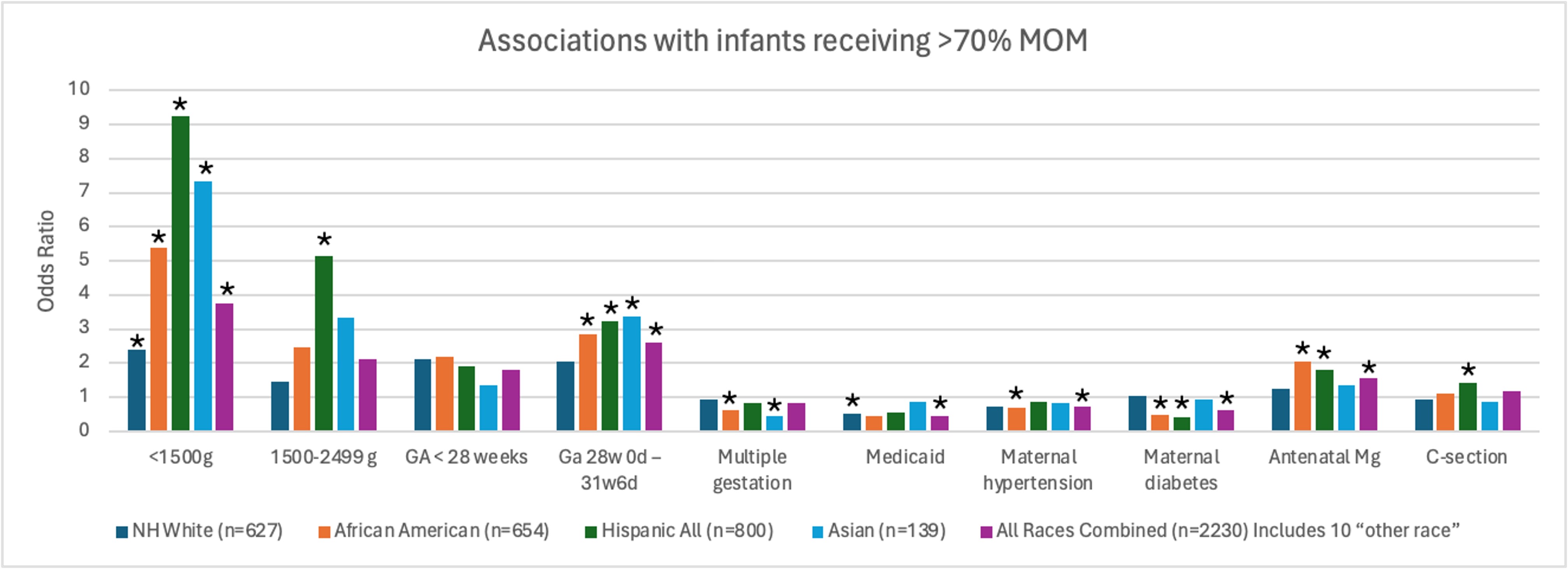 Odds of preterm infants receiving >70% MOM by Race and Ethnicity
Odds of preterm infants receiving >70% MOM by Race and Ethnicity.jpg) Odds of Preterm infants receiving <30% MOM by birthweight
Odds of Preterm infants receiving <30% MOM by birthweight