
Neonatal Fetal Nutrition & Metabolism 1
Session: Neonatal Fetal Nutrition & Metabolism 1
Dimitrios Angelis, MD
Neonatologist
University of Texas Southwestern Medical School
Dallas, Texas, United States
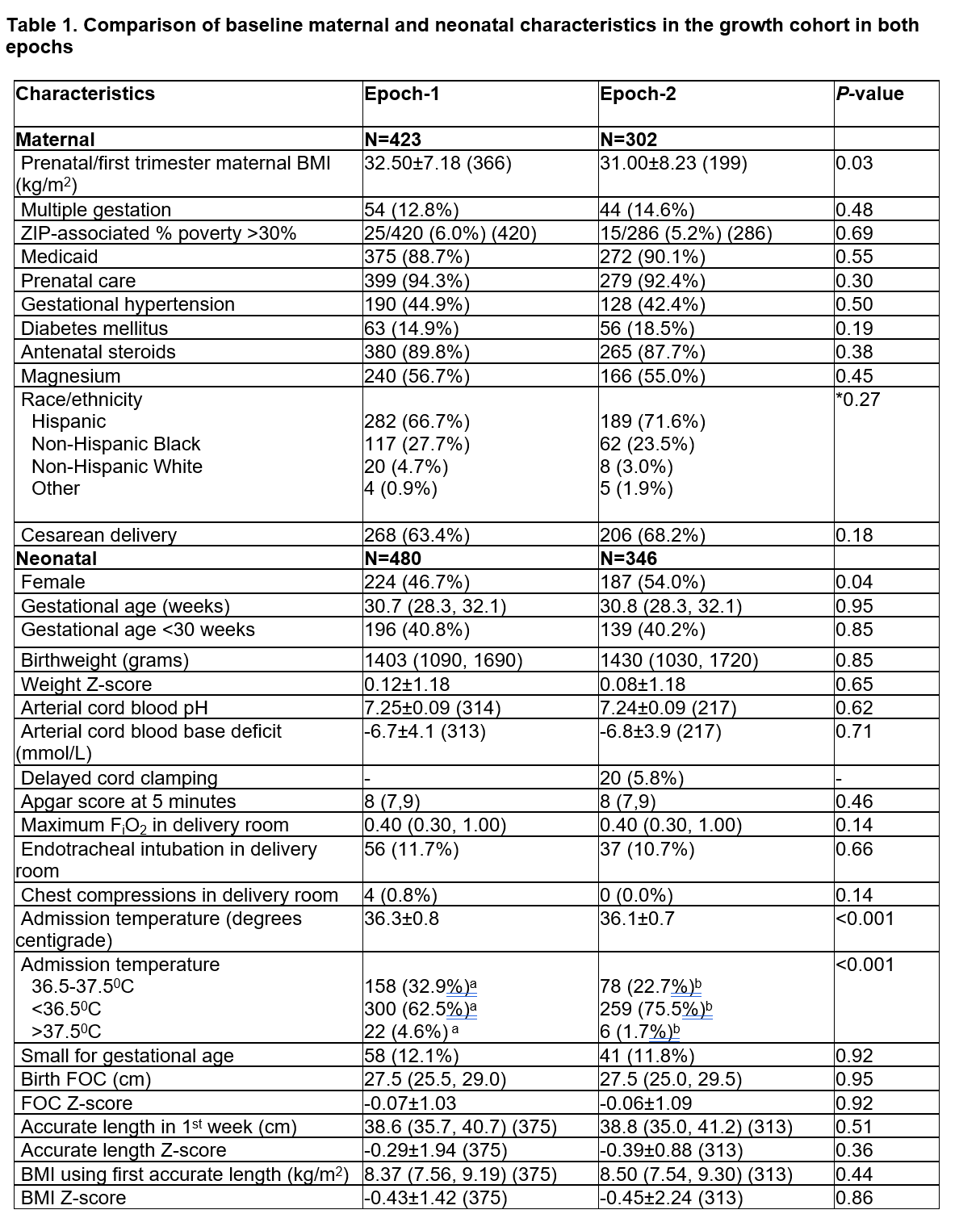 In Epoch-1, Zn supplementation in total parenteral nutrition (TPN) was 450 mcg/kg/day and enteral supplementation was provided only to those with documented Zn deficiency. In Epoch-2, Zn was provided with 500 mcg/kg/day in TPN and routine enteral supplementation, to achieve a total of 2.5 and later 2.7-3 mg/kg/day until 36 weeks postmenstrual age (PMA) or discharge. The discrepancy between the number of maternal and neonatal characteristics corresponds to multiple pregnancies.
In Epoch-1, Zn supplementation in total parenteral nutrition (TPN) was 450 mcg/kg/day and enteral supplementation was provided only to those with documented Zn deficiency. In Epoch-2, Zn was provided with 500 mcg/kg/day in TPN and routine enteral supplementation, to achieve a total of 2.5 and later 2.7-3 mg/kg/day until 36 weeks postmenstrual age (PMA) or discharge. The discrepancy between the number of maternal and neonatal characteristics corresponds to multiple pregnancies.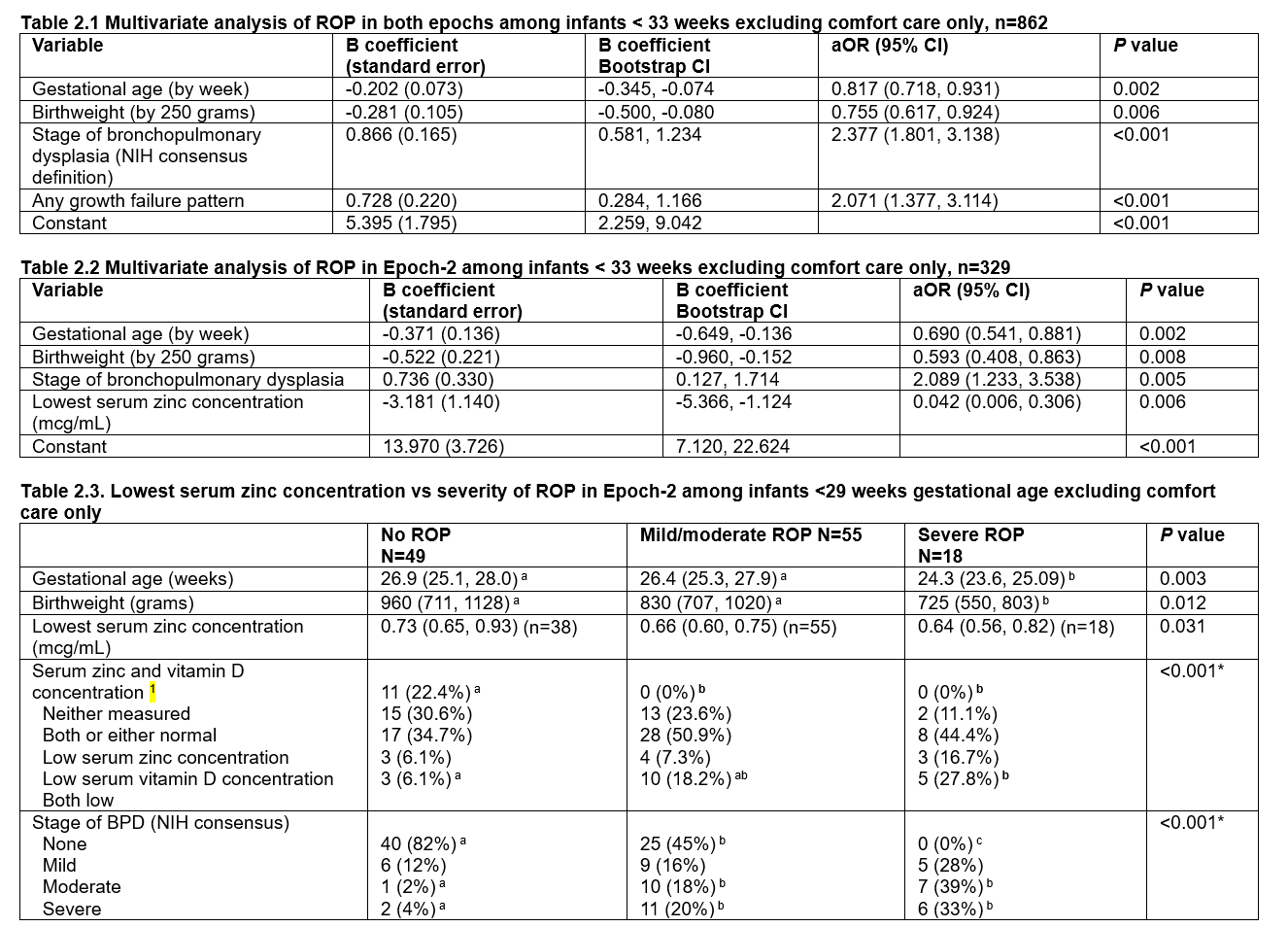 Table 2.1. Stepwise logistic regression analysis with bias-corrected accelerated 95% confidence intervals of the B coefficients was performed using 1000 bootstrap samples with SPSS: n=216 cases with ROP among 862 infants; Nagelkerke R2=0.472; Hosmer and Lemeshow test <0.001; AUROC=0.878 (95% CI 0.854, 0.902); Youden’s index 0.693 (predicted probability 0.140, sensitivity 0.907; specificity 0.686)
Table 2.1. Stepwise logistic regression analysis with bias-corrected accelerated 95% confidence intervals of the B coefficients was performed using 1000 bootstrap samples with SPSS: n=216 cases with ROP among 862 infants; Nagelkerke R2=0.472; Hosmer and Lemeshow test <0.001; AUROC=0.878 (95% CI 0.854, 0.902); Youden’s index 0.693 (predicted probability 0.140, sensitivity 0.907; specificity 0.686)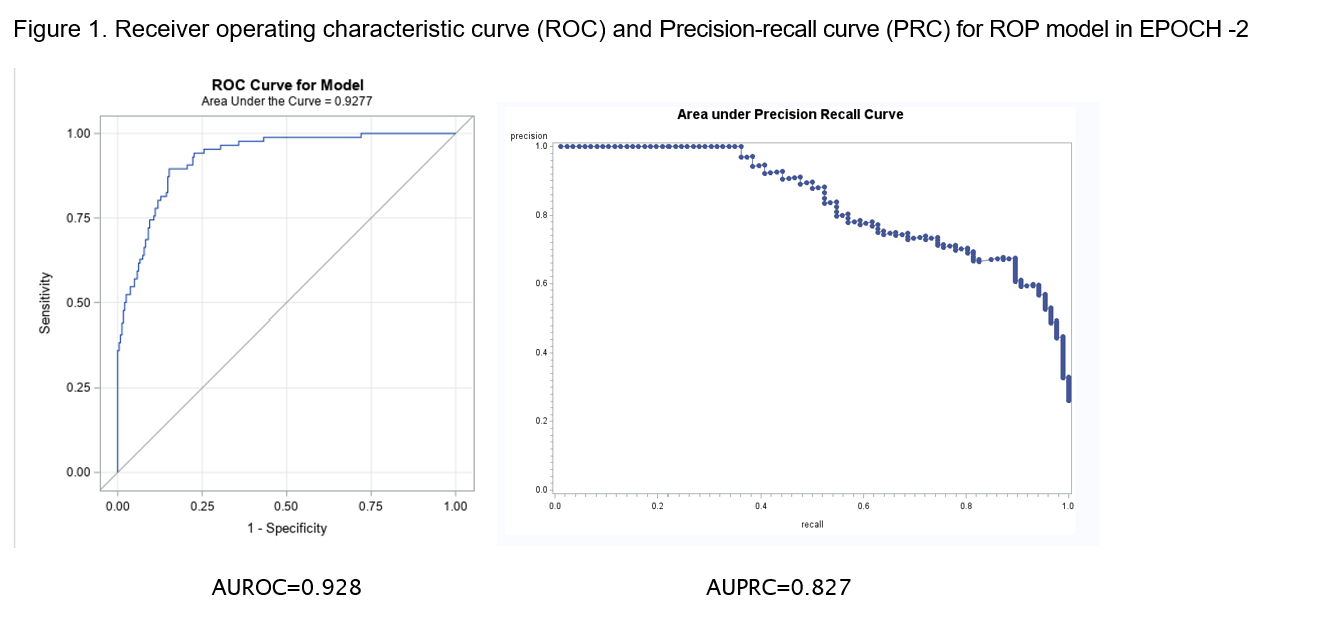 Abbreviations: AU: area under the curve; ROC Receiver operating characteristic curve; PRC: Precision-recall curve
Abbreviations: AU: area under the curve; ROC Receiver operating characteristic curve; PRC: Precision-recall curve 