
Breastfeeding/Human Milk 3
Session: Breastfeeding/Human Milk 3
.jpg "Igbagbosanmi Oredein, MD, MPH photo")
Igbagbosanmi Oredein, MD, MPH
Neonatal-Perinatal Medicine Fellow
Stanford University School of Medicine
Menlo Park, California, United States
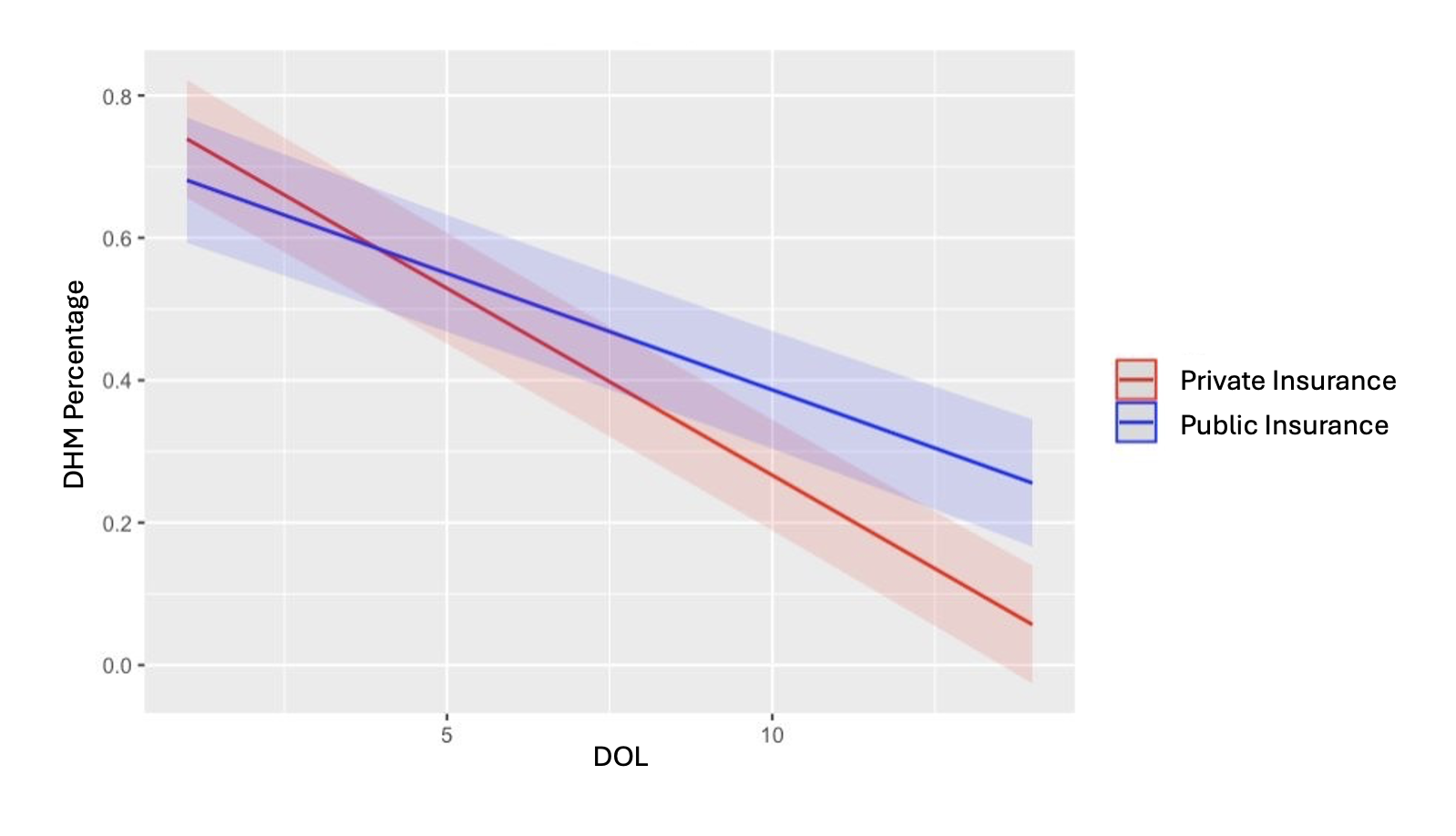 Modeled estimate of the interaction between Day of Life (DOL) and public insurance predicting Donor Human Milk (DHM) percentage while controlling for gestational age (GA)
Modeled estimate of the interaction between Day of Life (DOL) and public insurance predicting Donor Human Milk (DHM) percentage while controlling for gestational age (GA) 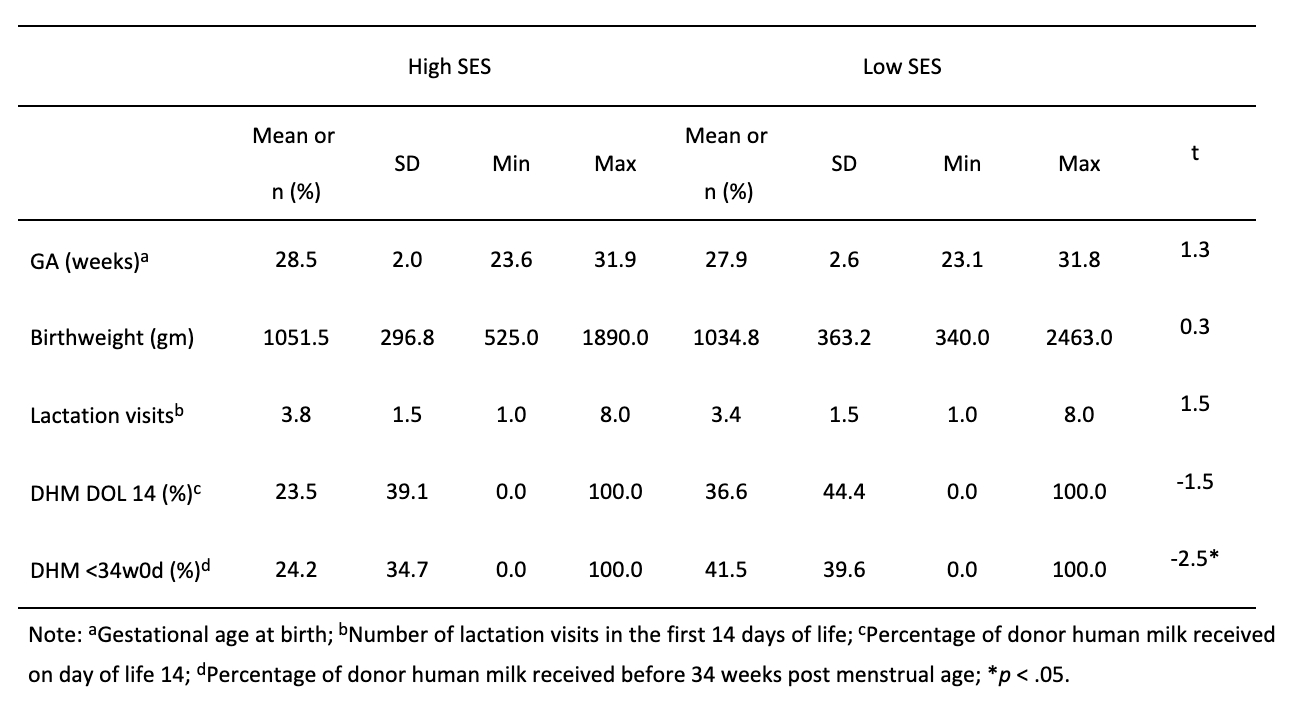 Comparison of clinical and demographic characteristics of infants in high- (n=67) vs. low-SES (n = 60) groups
Comparison of clinical and demographic characteristics of infants in high- (n=67) vs. low-SES (n = 60) groups 