
Health Services Research 1: Workforce & Underserved Areas
Session: Health Services Research 1: Workforce & Underserved Areas
 photo")
Colleen McLaughlin, MPH PhD (she/her/hers)
Research Scientist
Nationwide Children's Hospital
Columbus, Ohio, United States
 1. Medicaid/Child Health Insurance Program, United States, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, Washington
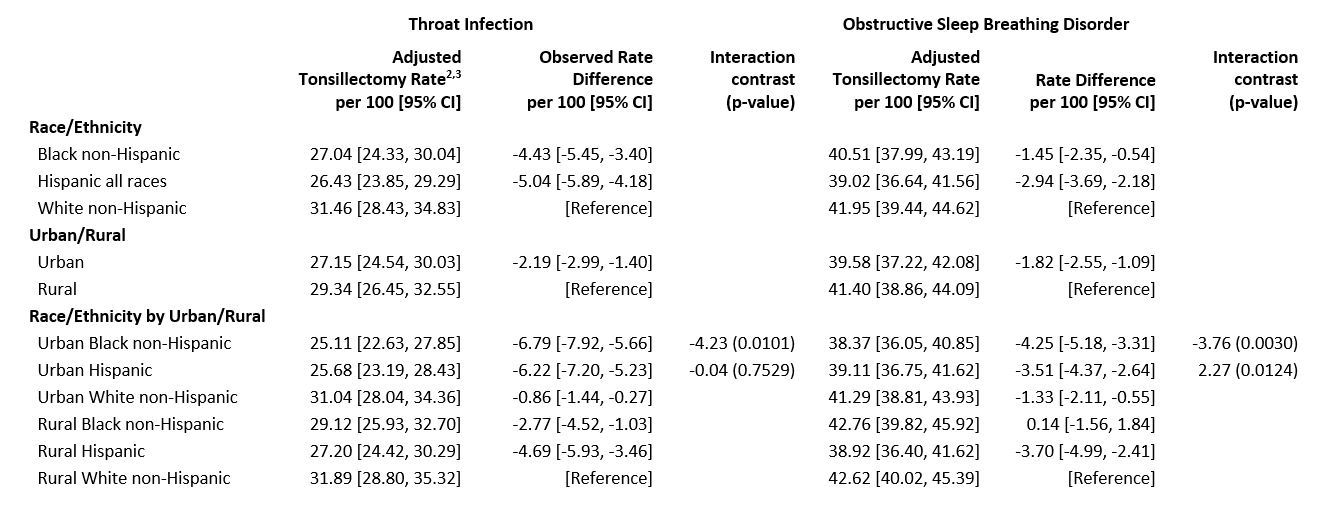
1. Medicaid/Child Health Insurance Program, United States, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, Washington 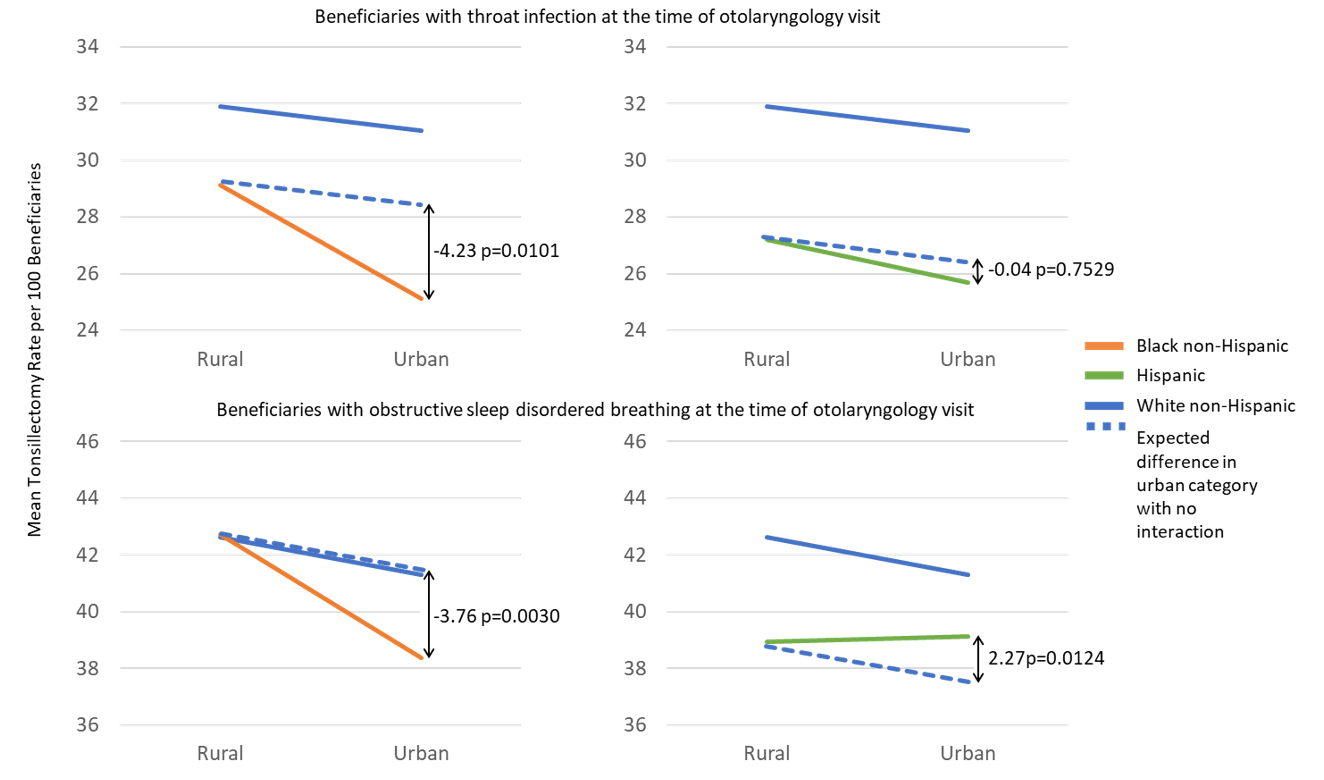 Medicaid/Child Health Insurance Program, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, and Washington. Rates are expressed as the percent of beneficiaries who had a tonsillectomy over 6 months of follow-up following otolaryngology visit, adjusted for State, sex, age, obesity, asthma, throat infection, attention deficit/hyperactivity disorder, and polysomnography before and after otolaryngology visit1. Medicaid/Child Health Insurance Program, United States, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, Washington Medicaid/Child Health Insurance Program, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, and Washington. Rates are expressed as the percent of beneficiaries who had a tonsillectomy over 6 months of follow-up following otolaryngology visit, adjusted for State, sex, age, obesity, asthma, throat infection, attention deficit/hyperactivity disorder, and polysomnography before and after otolaryngology visit
Medicaid/Child Health Insurance Program, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, and Washington. Rates are expressed as the percent of beneficiaries who had a tonsillectomy over 6 months of follow-up following otolaryngology visit, adjusted for State, sex, age, obesity, asthma, throat infection, attention deficit/hyperactivity disorder, and polysomnography before and after otolaryngology visit1. Medicaid/Child Health Insurance Program, United States, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, Washington Medicaid/Child Health Insurance Program, Jan 1, 2017-Jun 30, 2019, from California, Delaware, Florida, Indiana, Kentucky, Maine, North Carolina, New Hampshire, Nevada, Ohio, Oklahoma, Pennsylvania, South Dakota, Texas, and Washington. Rates are expressed as the percent of beneficiaries who had a tonsillectomy over 6 months of follow-up following otolaryngology visit, adjusted for State, sex, age, obesity, asthma, throat infection, attention deficit/hyperactivity disorder, and polysomnography before and after otolaryngology visit