
Neonatal Fetal Nutrition & Metabolism 1
Session: Neonatal Fetal Nutrition & Metabolism 1
Katie Huff, MD, MS (she/her/hers)
Assistant Professor of Clinical Pediatrics
Indiana University School of Medicine
Indianapolis, Indiana, United States
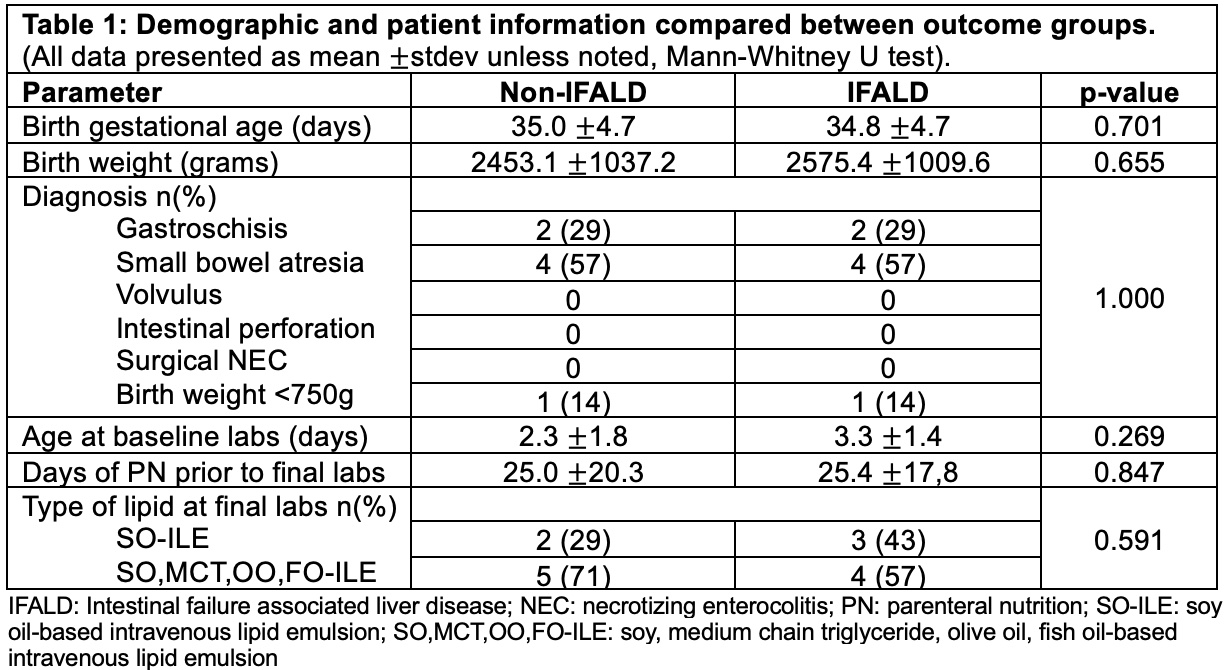 (All data presented as mean ±stdev unless noted, Mann-Whitney U test).
(All data presented as mean ±stdev unless noted, Mann-Whitney U test).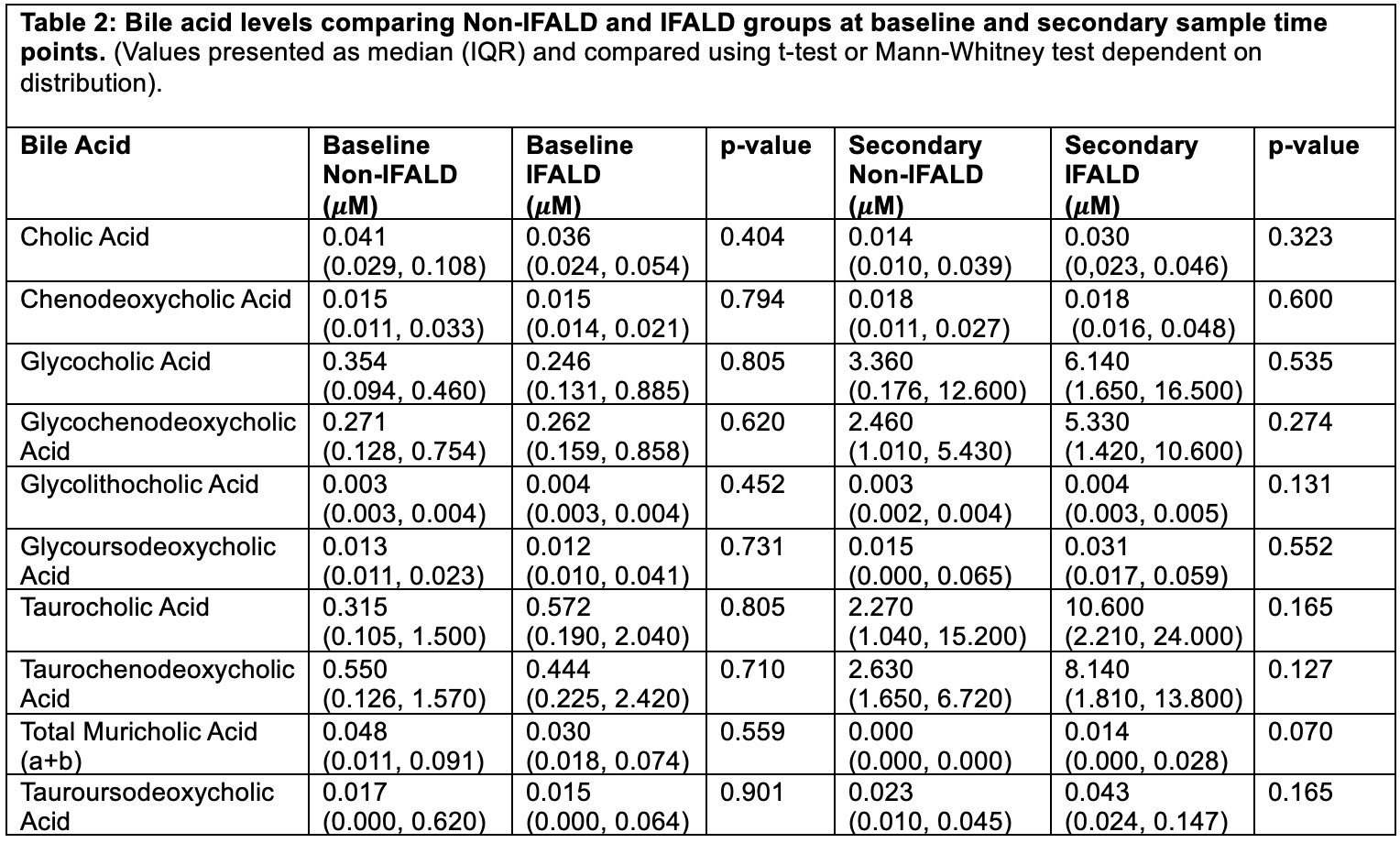 (Values presented as median (IQR) and compared using t-test or Mann-Whitney test dependent on distribution).
(Values presented as median (IQR) and compared using t-test or Mann-Whitney test dependent on distribution). 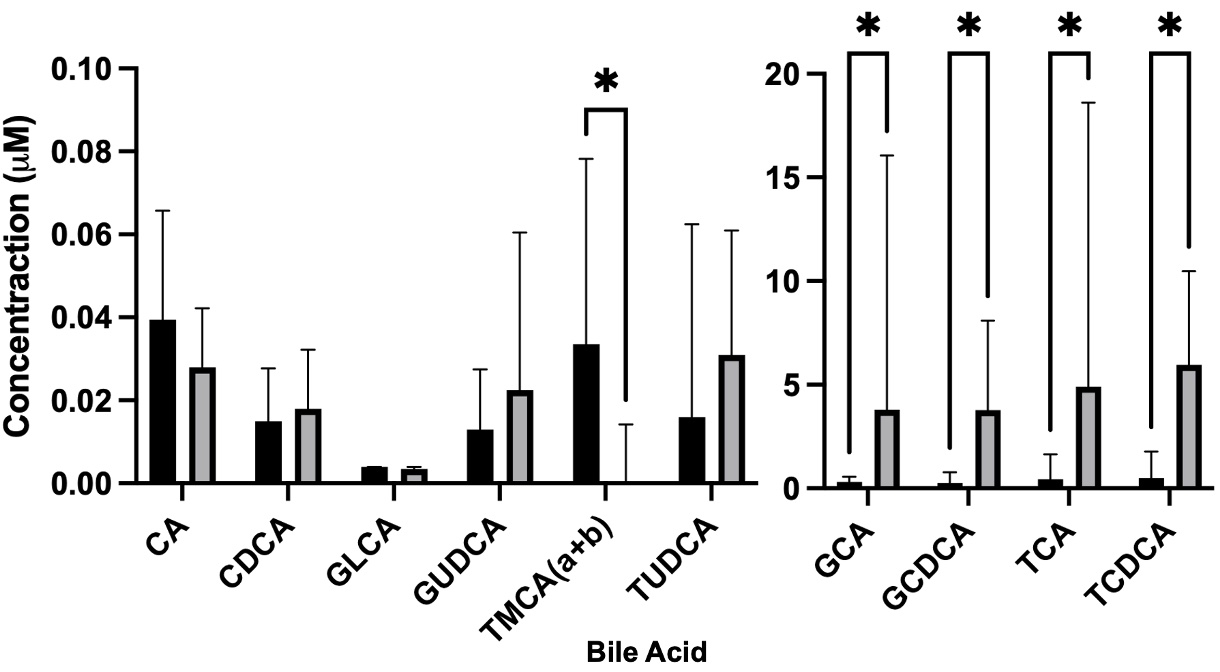 Two concentration intervals graphed to more accurately depict all bile acid levels. All values are represented as median and interquartile range. Asterisk notes comparisons significant at p-value <0.05. Mann-Whitney used for analysis. (CA: Cholic Acid; CDCA: Chenodeoxycholic Acid; GLCA: GCA: Glycocholic Acid; GCDCA: Glycochenodeoxycholic Acid; GLCA: Glycolithocholic Acid; GUDCA: Glycoursodeoxycholic Acid; TCA: Taurocholic Acid; TCDCA: Taurochenodeoxycholic Acid; TMCA (a+b): Total Muricholic Acid (a+b); TUDCA: Tauroursodeoxycholic Acid).
Two concentration intervals graphed to more accurately depict all bile acid levels. All values are represented as median and interquartile range. Asterisk notes comparisons significant at p-value <0.05. Mann-Whitney used for analysis. (CA: Cholic Acid; CDCA: Chenodeoxycholic Acid; GLCA: GCA: Glycocholic Acid; GCDCA: Glycochenodeoxycholic Acid; GLCA: Glycolithocholic Acid; GUDCA: Glycoursodeoxycholic Acid; TCA: Taurocholic Acid; TCDCA: Taurochenodeoxycholic Acid; TMCA (a+b): Total Muricholic Acid (a+b); TUDCA: Tauroursodeoxycholic Acid).