
Neonatal GI Physiology & NEC 1
Session: Neonatal GI Physiology & NEC 1
Ujjwala Mantha, MD (she/her/hers)
Fellow
The Hospital for Sick Children
Toronto, Ontario, Canada
.jpg) Abbreviations: PPROM: Premature prolonged rupture of membranes.
Abbreviations: PPROM: Premature prolonged rupture of membranes..jpg) Abbreviations: BPD-PH: bronchopulmonary dysplasia associated pulmonary hypertension, NEC: Necrotizing enterocolitis, NIV: Non-invasive ventilation, PMA: Post menstrual age, PNALD: Parenteral nutrition associated liver disease, ROP: Retinopathy of prematurity.
Abbreviations: BPD-PH: bronchopulmonary dysplasia associated pulmonary hypertension, NEC: Necrotizing enterocolitis, NIV: Non-invasive ventilation, PMA: Post menstrual age, PNALD: Parenteral nutrition associated liver disease, ROP: Retinopathy of prematurity.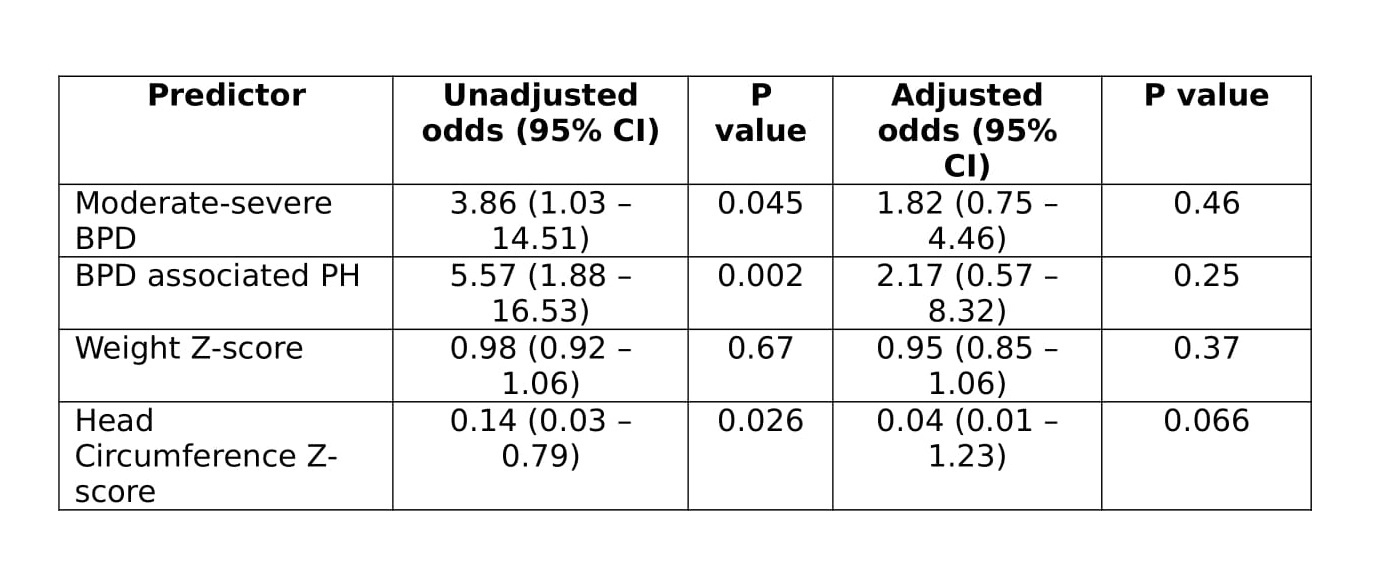 BPD – bronchopulmonary dysplasia, CI – confidence interval, PH – pulmonary hypertension
BPD – bronchopulmonary dysplasia, CI – confidence interval, PH – pulmonary hypertension