
Neonatal General 5: Infectious Disease and Immunology
Session: Neonatal General 5: Infectious Disease and Immunology
 photo")
Patricia Moran, MD (she/her/hers)
Neonatology Fellow
UVA
Charlottesville, Virginia, United States
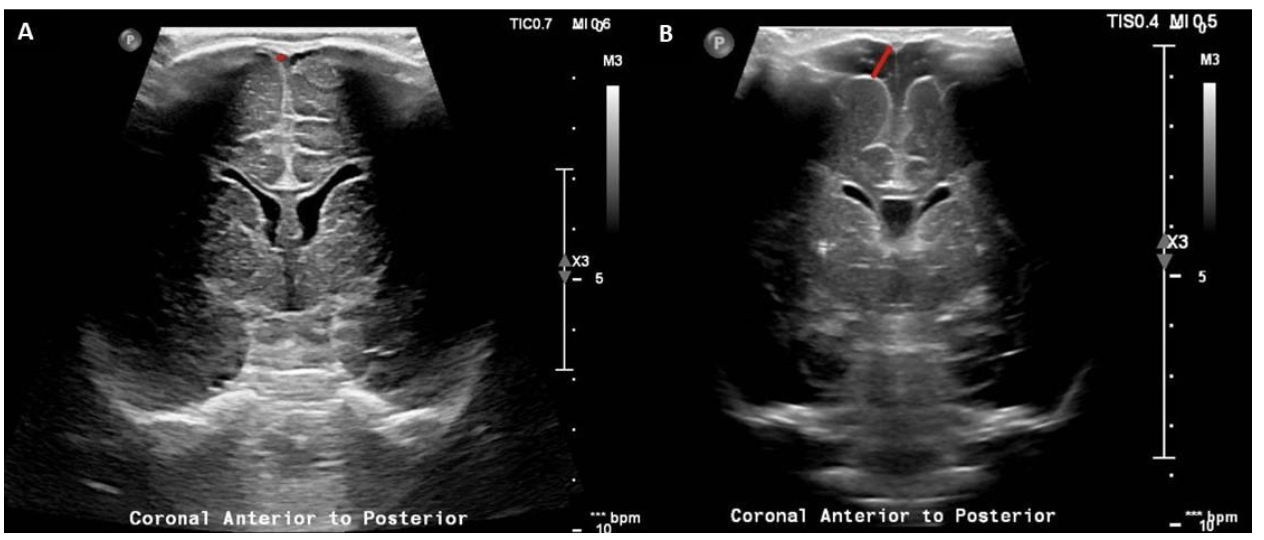 Panel A: Linear coronal view of a head ultrasound obtained at 44 weeks PMA in an infant born at 25 5/7 weeks and with a history of E-Coli early onset sepsis. SCW was measured to be 0.99 mm. Panel B: Linear coronal image of a head ultrasound obtained at 35 6/7 weeks PMA in an infant born at 25 6/7 weeks and with a history of Klebsiella late onset sepsis. SCW was measured to be 6.23 mm. Of note, all the measurements of SCW were obtained at the level of the foramen of Monro for standardization.
Panel A: Linear coronal view of a head ultrasound obtained at 44 weeks PMA in an infant born at 25 5/7 weeks and with a history of E-Coli early onset sepsis. SCW was measured to be 0.99 mm. Panel B: Linear coronal image of a head ultrasound obtained at 35 6/7 weeks PMA in an infant born at 25 6/7 weeks and with a history of Klebsiella late onset sepsis. SCW was measured to be 6.23 mm. Of note, all the measurements of SCW were obtained at the level of the foramen of Monro for standardization.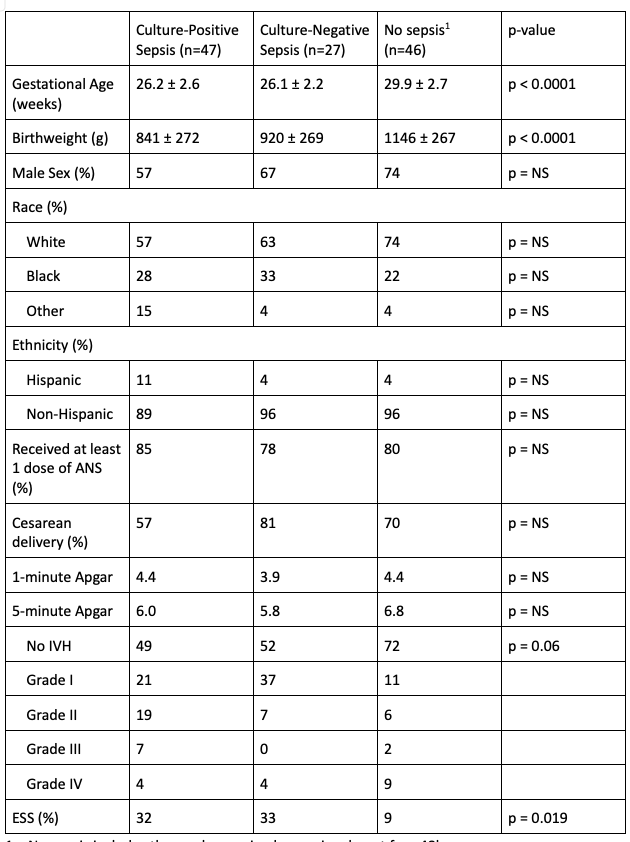 1 – No sepsis includes those who received a sepsis rule out for <48h.
1 – No sepsis includes those who received a sepsis rule out for <48h. 