
Emergency Medicine 5
Session: Emergency Medicine 5
 photo")
Simon Craig, MBBS FACEM MPH MHPE PhD (he/him/his)
Paediatric Emergency Physician / Adjunct Clinical Professor
Monash Health / Monash University
Clayton, Victoria, Australia
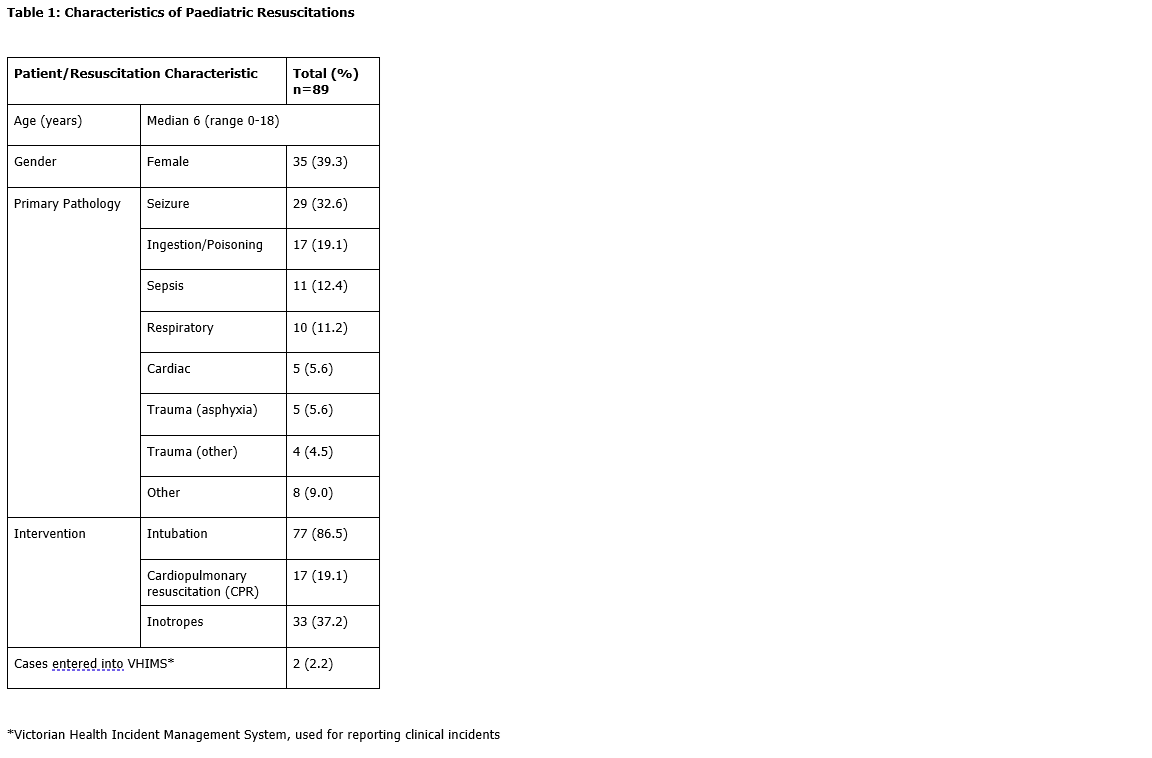 Characteristics of Paediatric Resuscitations
Characteristics of Paediatric Resuscitations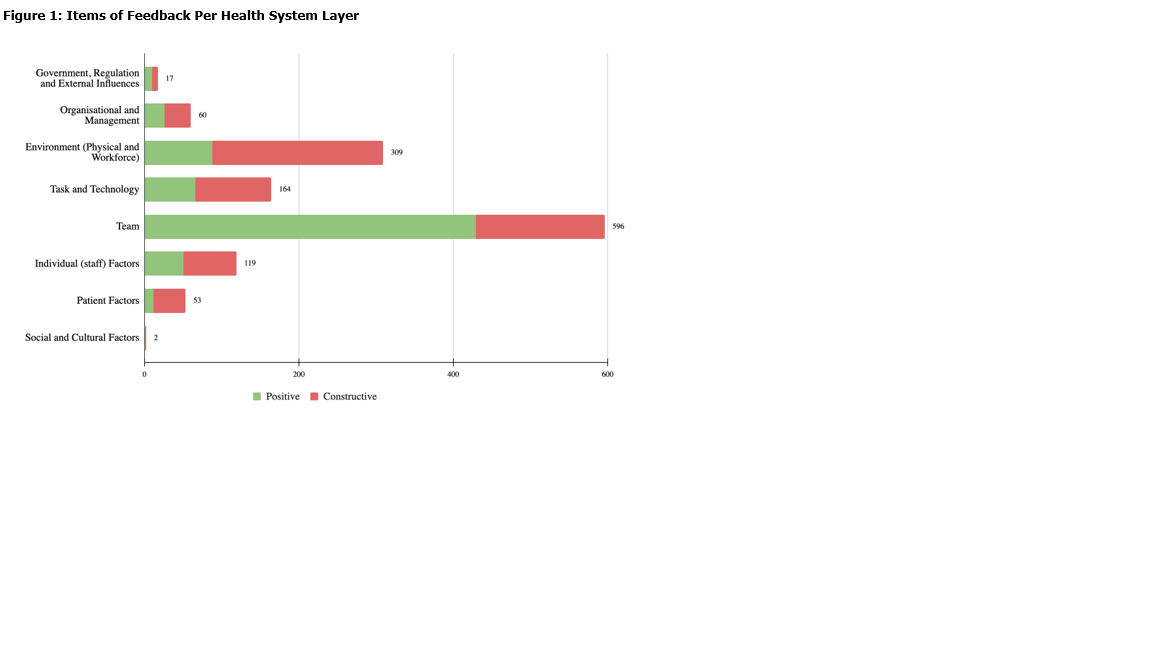 Items of Feedback Per Health System Layer
Items of Feedback Per Health System Layer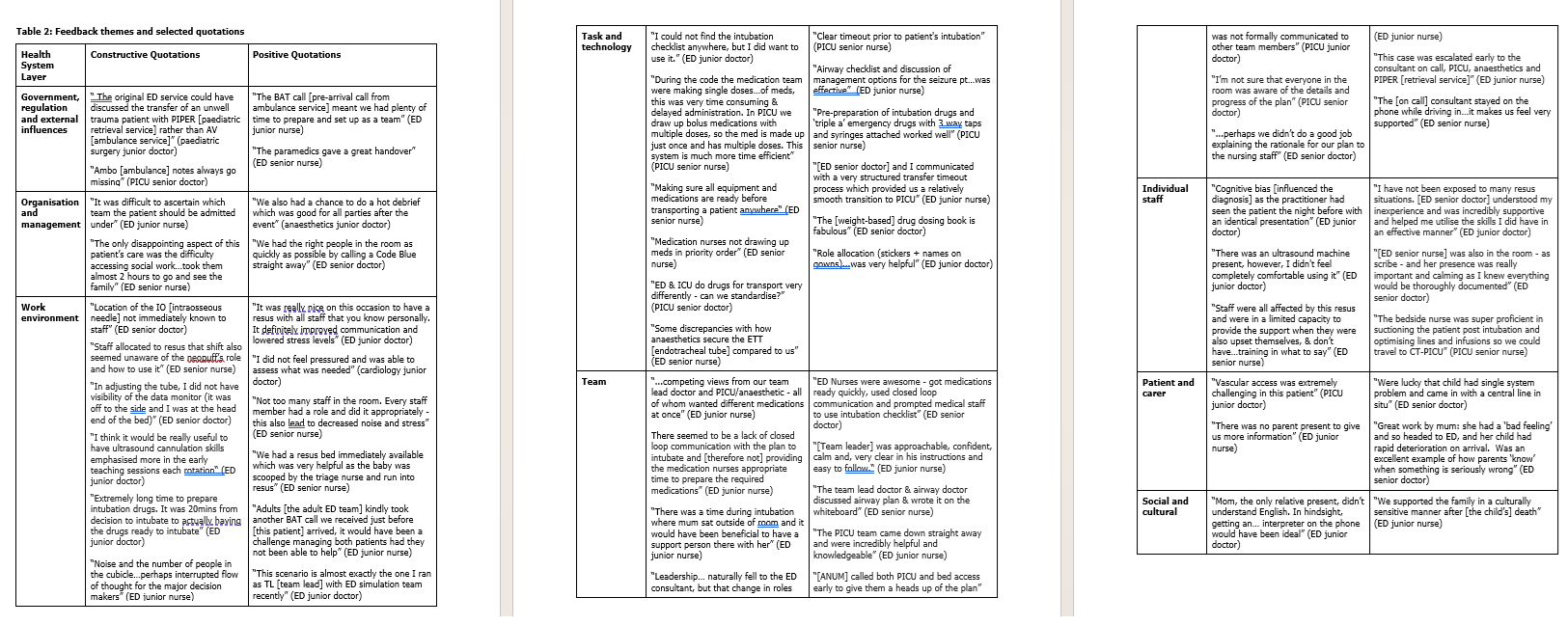 Feedback themes and selected quotations Characteristics of Paediatric ResuscitationsItems of Feedback Per Health System LayerFeedback themes and selected quotations
Feedback themes and selected quotations Characteristics of Paediatric ResuscitationsItems of Feedback Per Health System LayerFeedback themes and selected quotations 