Health Equity/Social Determinants of Health 2
Session: Health Equity/Social Determinants of Health 2
 photo")
Molly F. Lazarus, BA (she/her/hers)
Clinical Research Coordinator
Weill Cornell Medicine and Stanford Medicine
New York, New York, United States
.png) Note: *p < 0.05, **p < 0.01, ***p < 0.001.; Data are estimates (SE) of the fixed effects.
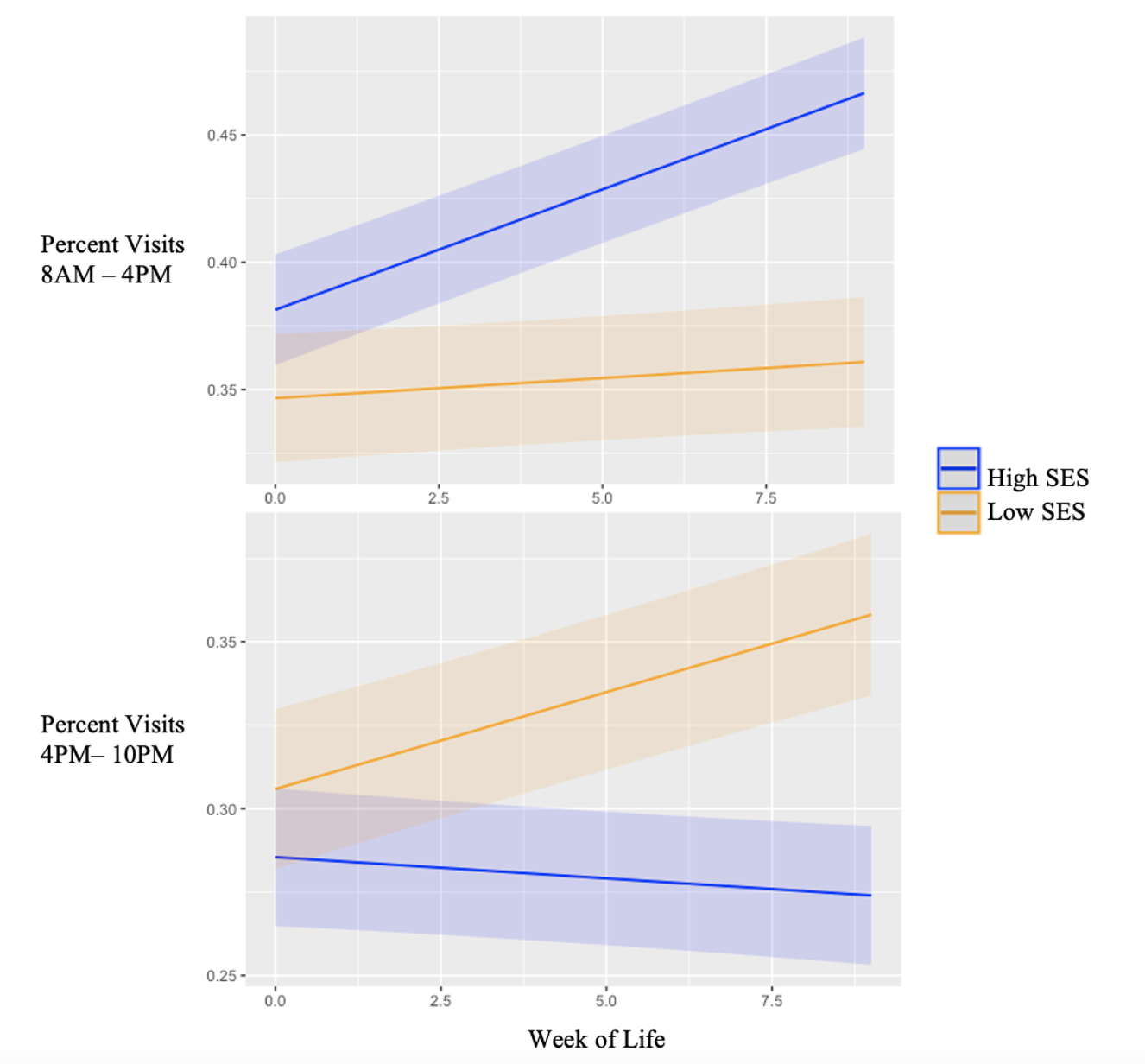
Note: *p < 0.05, **p < 0.01, ***p < 0.001.; Data are estimates (SE) of the fixed effects.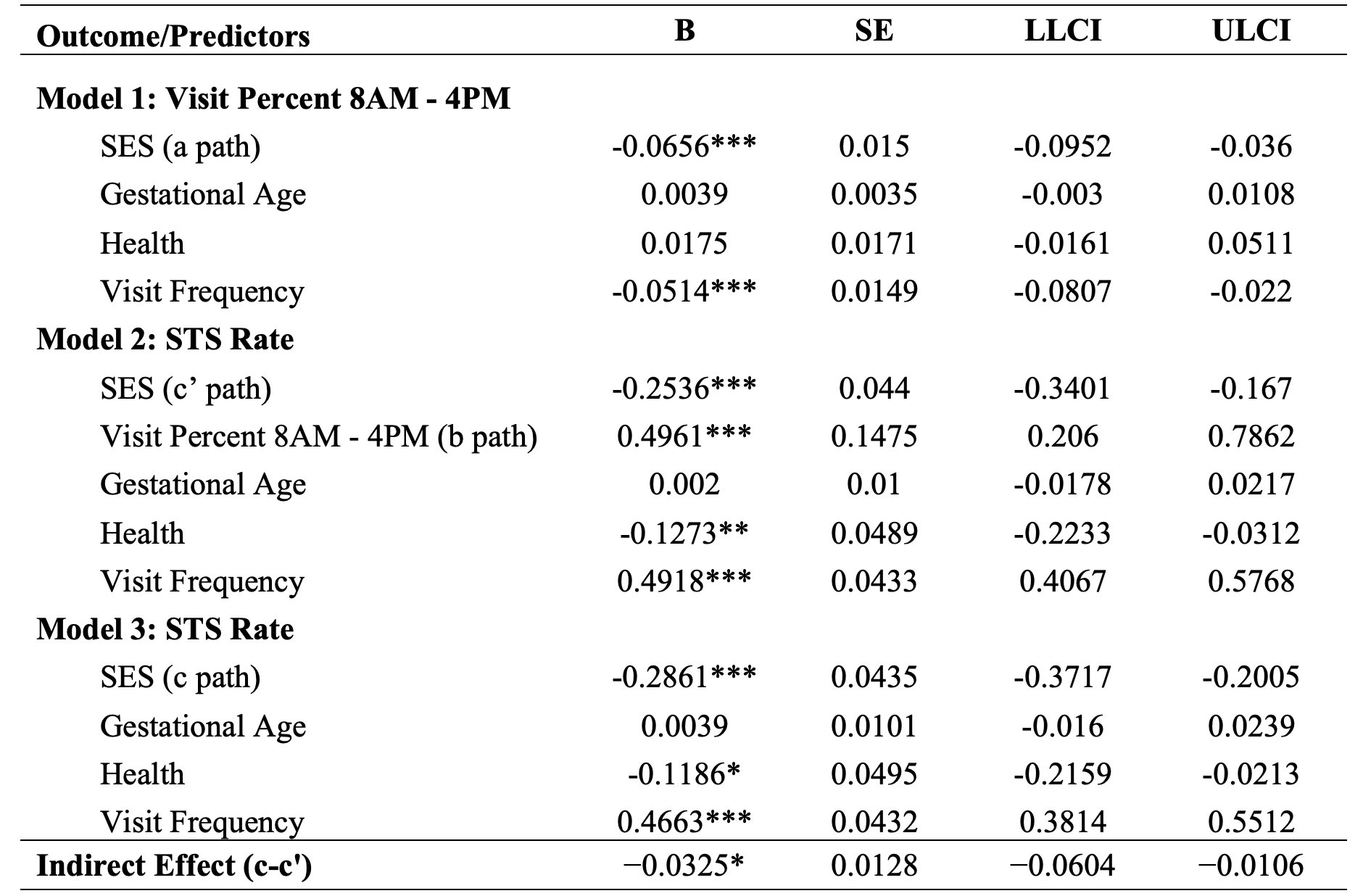 Note: p < .05*; p < .01**; p < .001***. Model 1 examines the relationship between SES and the mediator (daytime visitation), indicating that lower SES is associated with fewer family visits during the day (a path). Model 2 demonstrates that a higher percentage of daytime visitation is associated with increased engagement in skin-to-skin (STS) care, even when controlling for SES (b path). Models 2 and 3 show that SES predicts STS care rates, with lower SES families engaging in less skin-to-skin care (c and c’ paths). Critically, the analysis reveals a significant indirect effect of SES on STS care rate through reduced daytime visitation (c - c' path), suggesting that lower SES is linked to reduced STS care rates partly due to decreased family presence during the day.
Note: p < .05*; p < .01**; p < .001***. Model 1 examines the relationship between SES and the mediator (daytime visitation), indicating that lower SES is associated with fewer family visits during the day (a path). Model 2 demonstrates that a higher percentage of daytime visitation is associated with increased engagement in skin-to-skin (STS) care, even when controlling for SES (b path). Models 2 and 3 show that SES predicts STS care rates, with lower SES families engaging in less skin-to-skin care (c and c’ paths). Critically, the analysis reveals a significant indirect effect of SES on STS care rate through reduced daytime visitation (c - c' path), suggesting that lower SES is linked to reduced STS care rates partly due to decreased family presence during the day.