
Emergency Medicine 5
Session: Emergency Medicine 5
 Credit")
 photo")
Collin Huth, MD (he/him/his)
Resident
UH Rainbow Babies & Children's Hospital
Cleveland, Ohio, United States
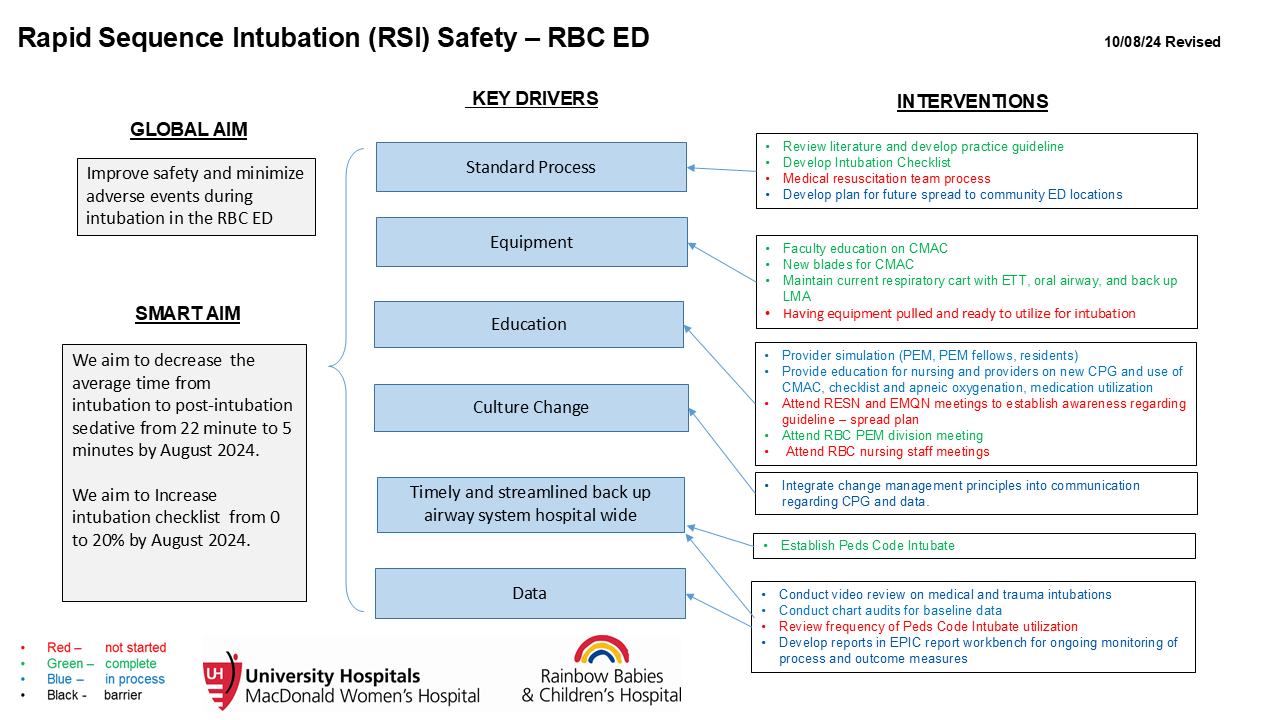 Key Driver Diagram
Key Driver Diagram.png) Front of our Intubation Checklist.
Front of our Intubation Checklist.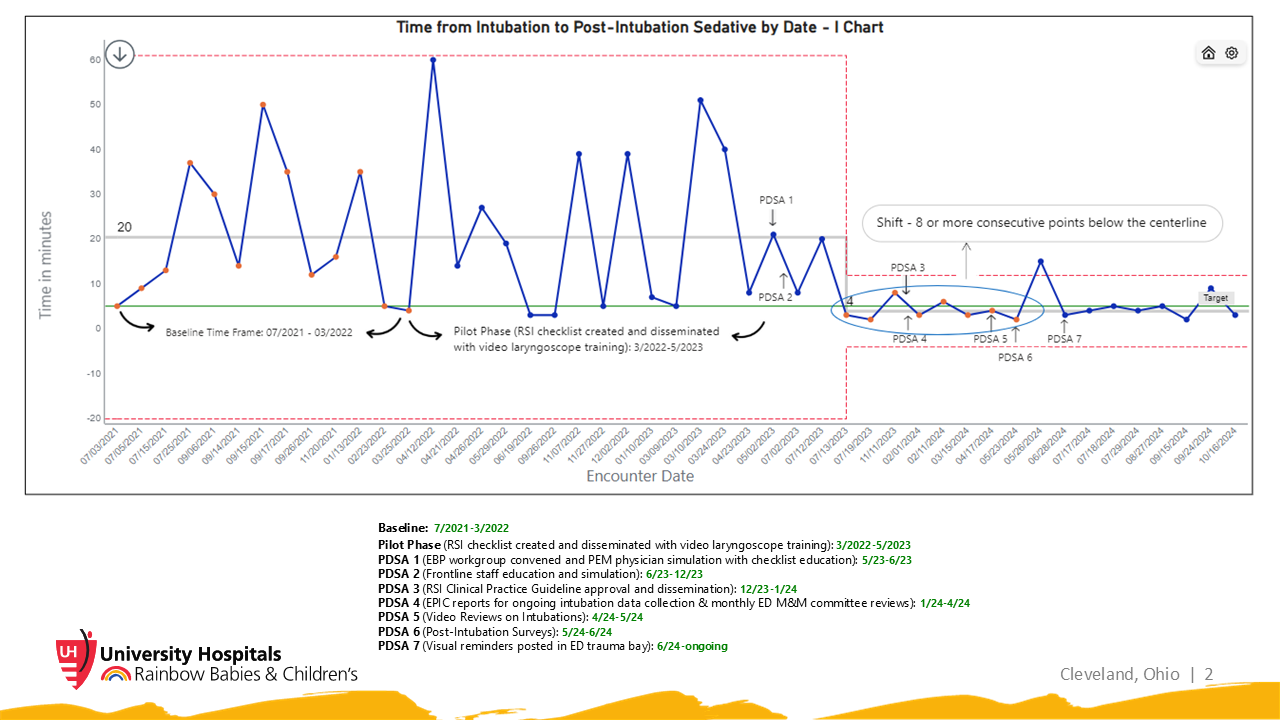 I-Chart with annotations detailing timeline of PDSA cycles. Special cause variation noted between PDSA cycles 3 and 4.
I-Chart with annotations detailing timeline of PDSA cycles. Special cause variation noted between PDSA cycles 3 and 4.