
Technology 2: Telemedicine
Session: Technology 2: Telemedicine
 photo")
Jennifer C. Keene, MD, MS, MBA (she/her/hers)
Assistant professor of neonatal neurology
University of Utah
Salt Lake City, Utah, United States
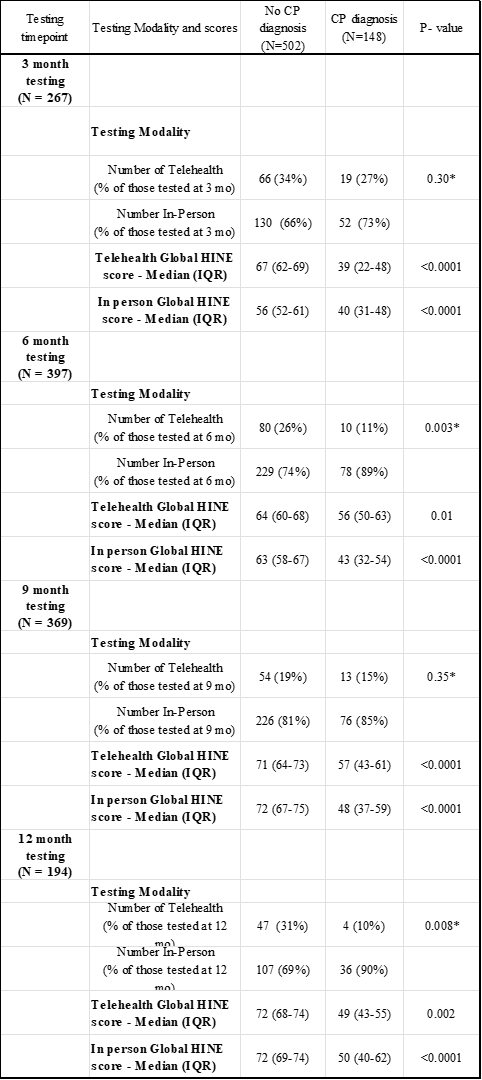 CP - Cerebral Palsy, HINE - Hammersmith Infant Neurologic Exam, IQR - Interquartile range (25%ile - 75%ile), * p-value calculated for overall Fisher's exact comparison between patients who do and do not have CP
CP - Cerebral Palsy, HINE - Hammersmith Infant Neurologic Exam, IQR - Interquartile range (25%ile - 75%ile), * p-value calculated for overall Fisher's exact comparison between patients who do and do not have CP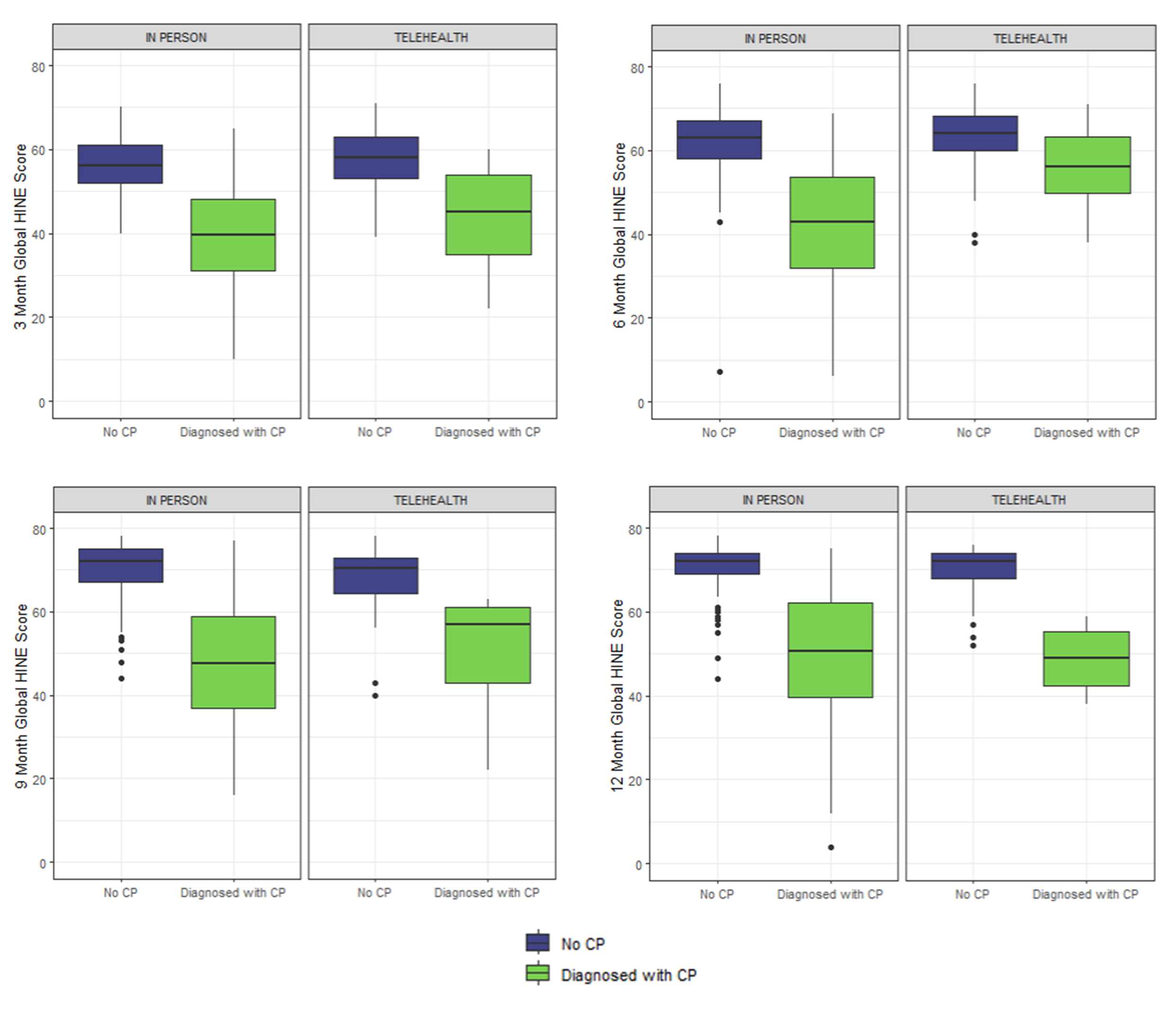 Comparison of Global Hammersmith Infant Neurologic Exam (HINE) scores at 3, 6, 9 and 12 months for patients with vs without CP for visits that were conducted either in-person or via telehealth exam. Global HINE scores were significantly different for patients with and without CP at all time timepoints and by both exam modalities
Comparison of Global Hammersmith Infant Neurologic Exam (HINE) scores at 3, 6, 9 and 12 months for patients with vs without CP for visits that were conducted either in-person or via telehealth exam. Global HINE scores were significantly different for patients with and without CP at all time timepoints and by both exam modalities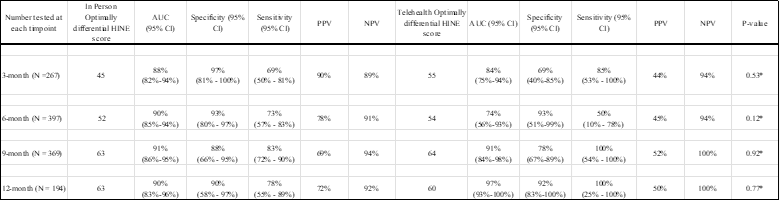 AUC = Area Under Curve, CI - Confidence Interval, HINE - Hammersmith Infant Neurologic Exam, IQR - Interquartile range (25%ile - 75%ile), NPV = Negative predictive value, PPV = Positive predictive value, * p-value calculated for the comparison of AUC between Telehealth and In-Person HINE exams
AUC = Area Under Curve, CI - Confidence Interval, HINE - Hammersmith Infant Neurologic Exam, IQR - Interquartile range (25%ile - 75%ile), NPV = Negative predictive value, PPV = Positive predictive value, * p-value calculated for the comparison of AUC between Telehealth and In-Person HINE exams