
Emergency Medicine 4
Session: Emergency Medicine 4
 photo")
Sofia S. Cook, MD (she/her/hers)
Pediatric Emergency Medicine Fellow
Children's Hospital Los Angeles
Los Angeles, California, United States
.jpg) (A) This is an example of a picture-based asthma action plan (PB-AAP) in English for a young child who has no prescriptions for daily asthma preventer medications and requires a spacer with a mask for inhaled medications. (B) This is an example of a PB-AAP in Spanish for an older child who has prescriptions for daily asthma preventer medications and can use a spacer without a mask for inhaled medications. Note: The pediatric emergency medicine (PEM) attending or fellow first complete the W-AAP in the patient’s chart. Based on the W-AAP, a unique version of the PB-AAP in the desired language is created to reflect medication formulations, method of delivery, frequency of use, etc. Medication names and dosages are directly transcribed from the standard AAP onto the PB-AAP. Any medication questions or discrepancies are directly reviewed with the PEM attending and/or fellow.
(A) This is an example of a picture-based asthma action plan (PB-AAP) in English for a young child who has no prescriptions for daily asthma preventer medications and requires a spacer with a mask for inhaled medications. (B) This is an example of a PB-AAP in Spanish for an older child who has prescriptions for daily asthma preventer medications and can use a spacer without a mask for inhaled medications. Note: The pediatric emergency medicine (PEM) attending or fellow first complete the W-AAP in the patient’s chart. Based on the W-AAP, a unique version of the PB-AAP in the desired language is created to reflect medication formulations, method of delivery, frequency of use, etc. Medication names and dosages are directly transcribed from the standard AAP onto the PB-AAP. Any medication questions or discrepancies are directly reviewed with the PEM attending and/or fellow. 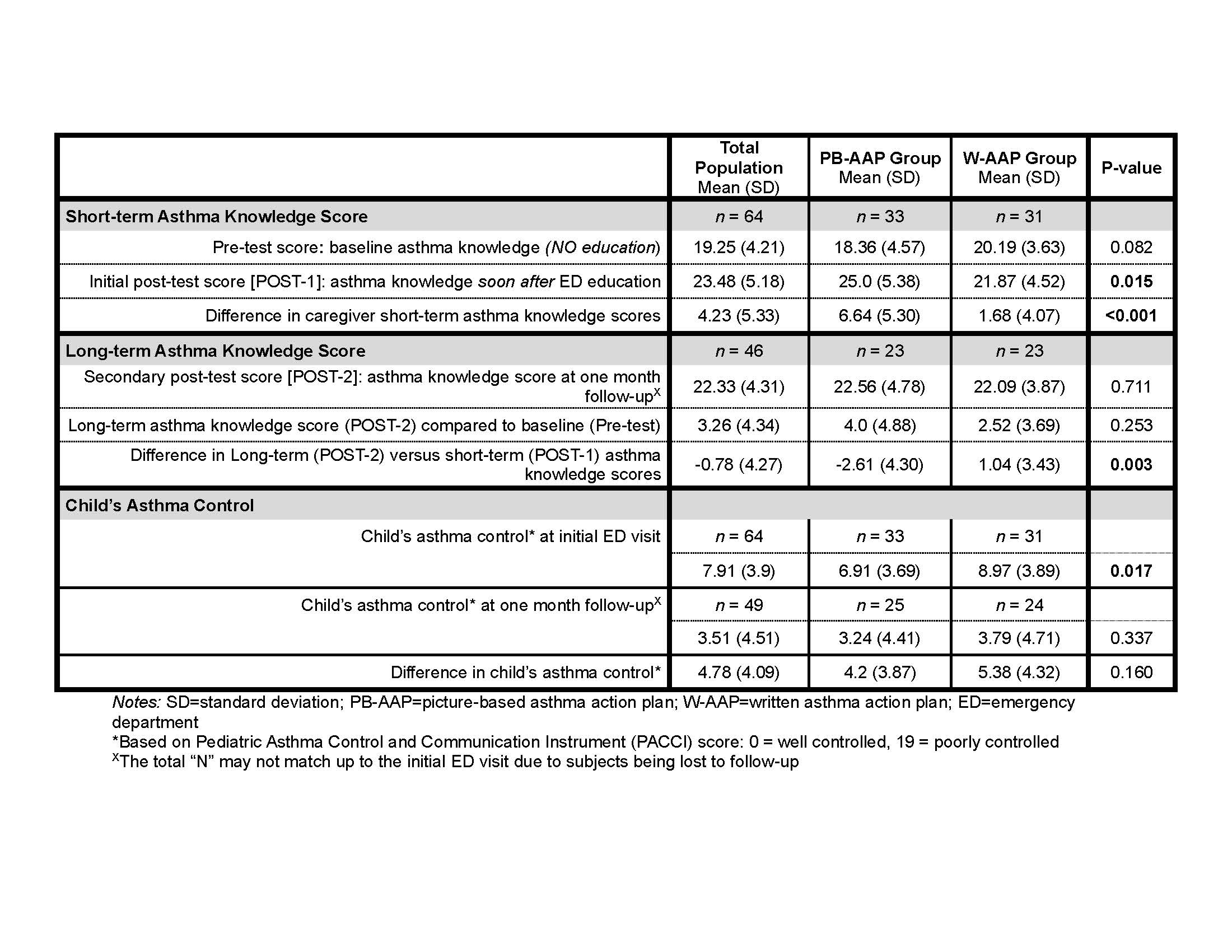 Caregiver’s asthma knowledge scores and child’s asthma control by randomization group
Caregiver’s asthma knowledge scores and child’s asthma control by randomization group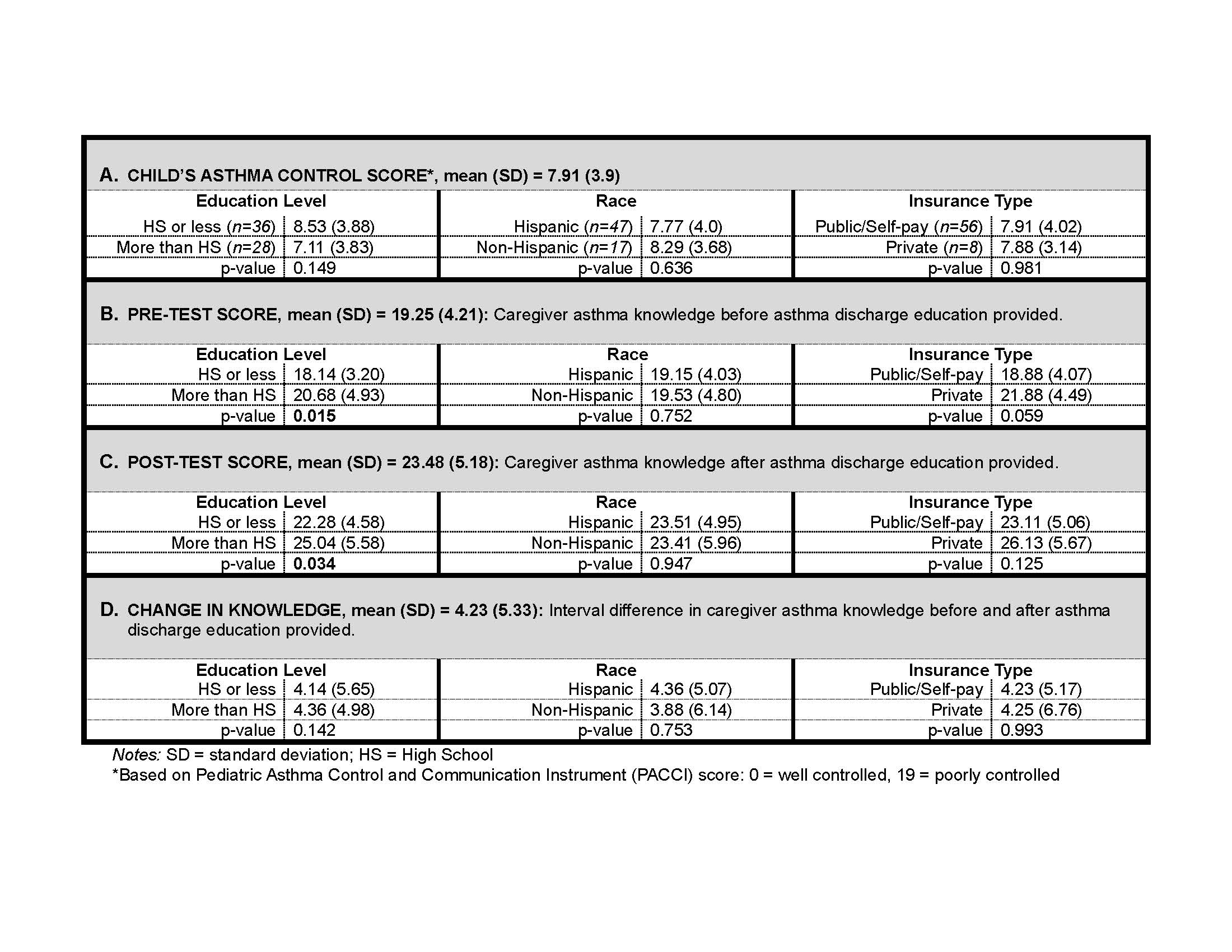 Disparities in child’s asthma control and caregiver’s asthma knowledge scores by caregiver’s highest education level, caregiver’s race, and child’s insurance type (N=64)(A) This is an example of a picture-based asthma action plan (PB-AAP) in English for a young child who has no prescriptions for daily asthma preventer medications and requires a spacer with a mask for inhaled medications. (B) This is an example of a PB-AAP in Spanish for an older child who has prescriptions for daily asthma preventer medications and can use a spacer without a mask for inhaled medications. Note: The pediatric emergency medicine (PEM) attending or fellow first complete the W-AAP in the patient’s chart. Based on the W-AAP, a unique version of the PB-AAP in the desired language is created to reflect medication formulations, method of delivery, frequency of use, etc. Medication names and dosages are directly transcribed from the standard AAP onto the PB-AAP. Any medication questions or discrepancies are directly reviewed with the PEM attending and/or fellow. Caregiver’s asthma knowledge scores and child’s asthma control by randomization groupDisparities in child’s asthma control and caregiver’s asthma knowledge scores by caregiver’s highest education level, caregiver’s race, and child’s insurance type (N=64)
Disparities in child’s asthma control and caregiver’s asthma knowledge scores by caregiver’s highest education level, caregiver’s race, and child’s insurance type (N=64)(A) This is an example of a picture-based asthma action plan (PB-AAP) in English for a young child who has no prescriptions for daily asthma preventer medications and requires a spacer with a mask for inhaled medications. (B) This is an example of a PB-AAP in Spanish for an older child who has prescriptions for daily asthma preventer medications and can use a spacer without a mask for inhaled medications. Note: The pediatric emergency medicine (PEM) attending or fellow first complete the W-AAP in the patient’s chart. Based on the W-AAP, a unique version of the PB-AAP in the desired language is created to reflect medication formulations, method of delivery, frequency of use, etc. Medication names and dosages are directly transcribed from the standard AAP onto the PB-AAP. Any medication questions or discrepancies are directly reviewed with the PEM attending and/or fellow. Caregiver’s asthma knowledge scores and child’s asthma control by randomization groupDisparities in child’s asthma control and caregiver’s asthma knowledge scores by caregiver’s highest education level, caregiver’s race, and child’s insurance type (N=64)