
Emergency Medicine 6
Session: Emergency Medicine 6
 Credit")
Jennifer Thull-Freedman, MD, MSc
Clinical Professor
University of Calgary
Calgary, Alberta, Canada
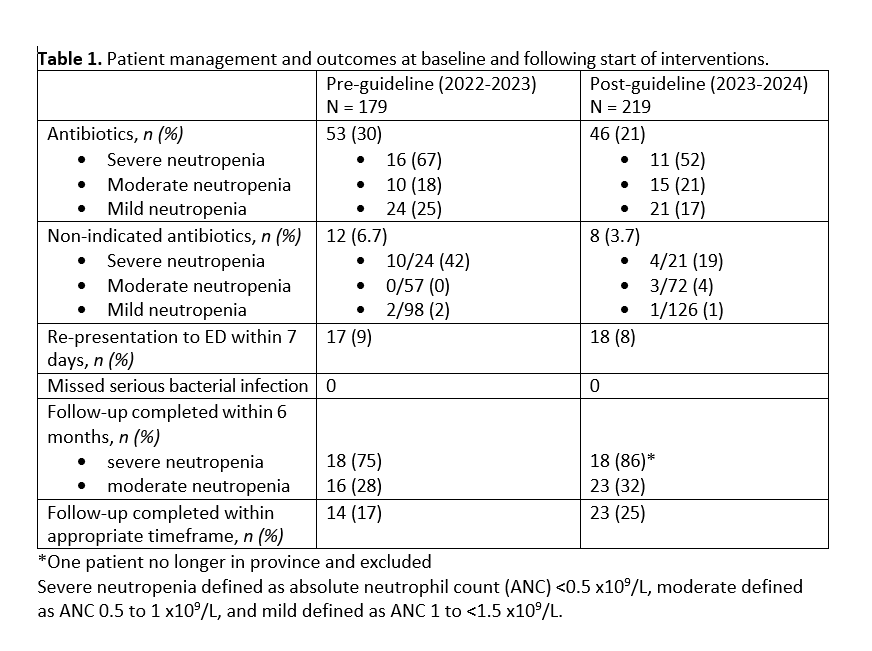 Management of ED patients with febrile neutropenia before and after the start of interventions
Management of ED patients with febrile neutropenia before and after the start of interventions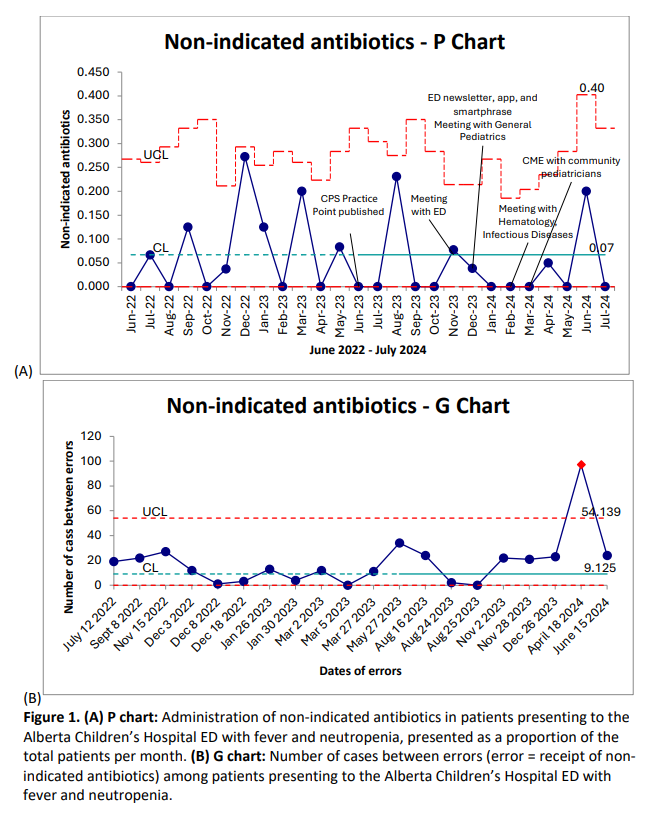 P-chart and G-chart for primary outcome of proportion of otherwise well children with febrile neutropenia receiving non-indicated antibiotics in the ED. G-chart demonstrated number of cases appropriately treated between occurrences of inappropriate treatment.
P-chart and G-chart for primary outcome of proportion of otherwise well children with febrile neutropenia receiving non-indicated antibiotics in the ED. G-chart demonstrated number of cases appropriately treated between occurrences of inappropriate treatment. 