
Emergency Medicine 5
Session: Emergency Medicine 5
 photo")
Mariju Baluyot, MD (she/her/hers)
Assistant Professor of Clinical Emergency Medicine and Pediatrics
Riley Hospital for Children at Indiana University Health
Fishers, Indiana, United States
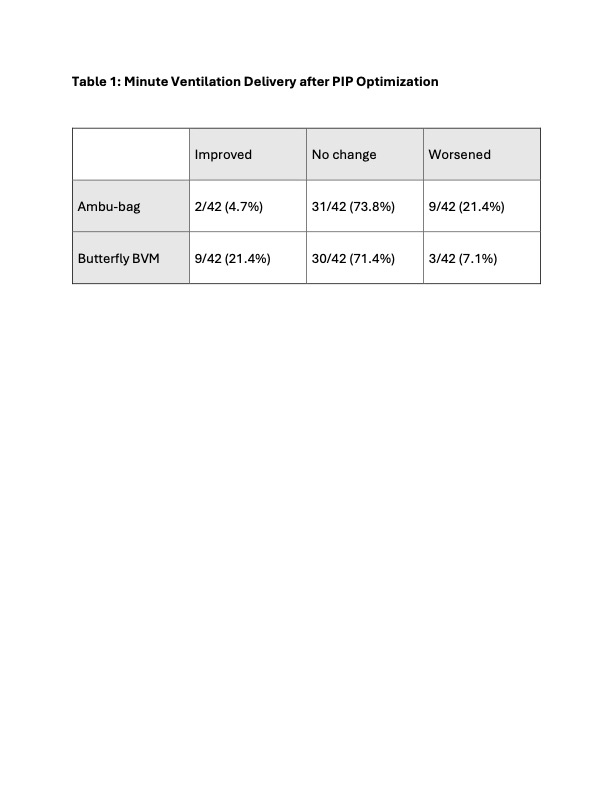 Table 1: Minute Ventilation Delivery after PIP Optimization
Table 1: Minute Ventilation Delivery after PIP Optimization 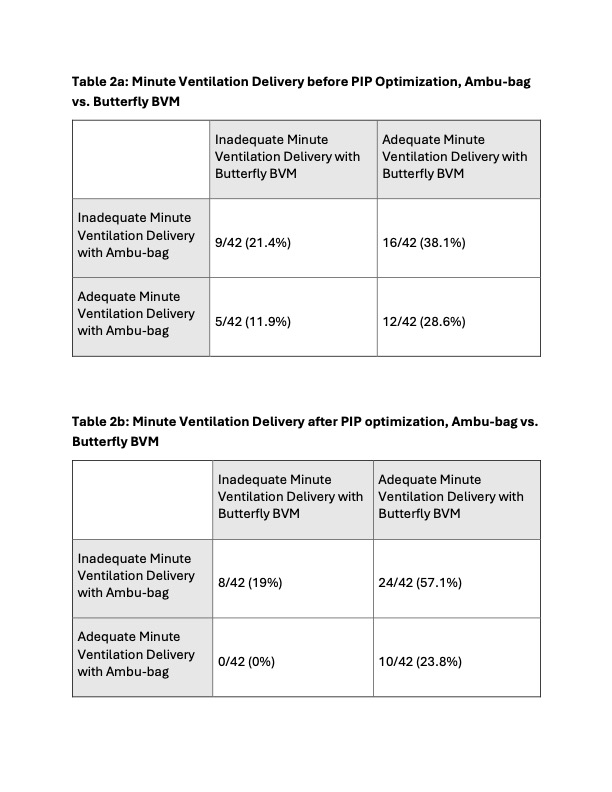 Table 2a: Minute Ventilation Delivery before PIP Optimization, Ambu-bag vs. Butterfly BVM; Table 2b: Minute Ventilation Delivery after PIP optimization, Ambu-bag vs. Butterfly BVM Table 1: Minute Ventilation Delivery after PIP Optimization Table 2a: Minute Ventilation Delivery before PIP Optimization, Ambu-bag vs. Butterfly BVM; Table 2b: Minute Ventilation Delivery after PIP optimization, Ambu-bag vs. Butterfly BVM
Table 2a: Minute Ventilation Delivery before PIP Optimization, Ambu-bag vs. Butterfly BVM; Table 2b: Minute Ventilation Delivery after PIP optimization, Ambu-bag vs. Butterfly BVM Table 1: Minute Ventilation Delivery after PIP Optimization Table 2a: Minute Ventilation Delivery before PIP Optimization, Ambu-bag vs. Butterfly BVM; Table 2b: Minute Ventilation Delivery after PIP optimization, Ambu-bag vs. Butterfly BVM 