
Neonatal Hemodynamics and Cardiovascular Medicine 3
Session: Neonatal Hemodynamics and Cardiovascular Medicine 3

Mahati Pidaparti, MD
Fellow
Indiana University School of Medicine
Indianapolis, Indiana, United States
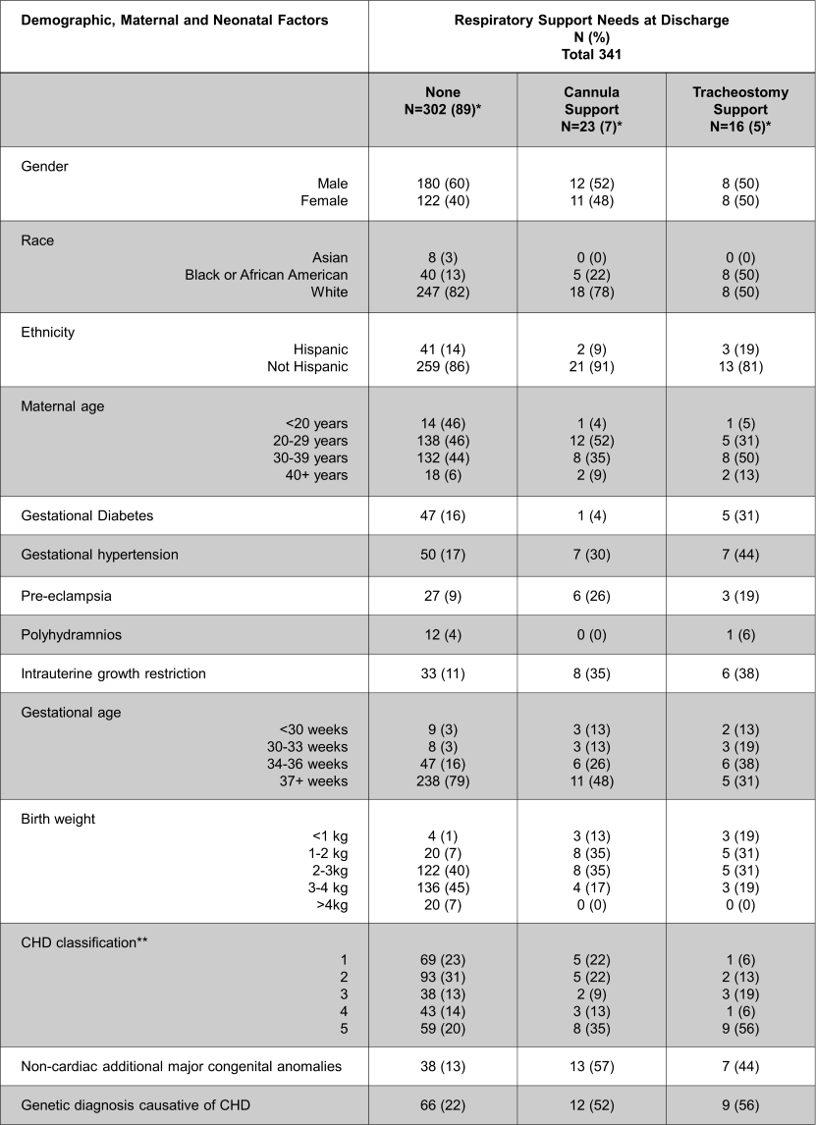 *Percentages may not total to 100 due to missing values.
*Percentages may not total to 100 due to missing values. 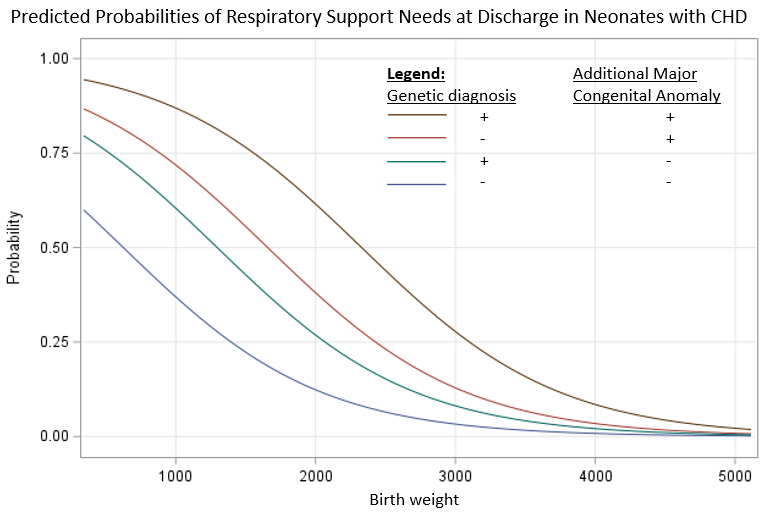 Predicted probabilities of respiratory support at discharge based on birth weight, genetic diagnosis causative of CHD, and additional major congenital anomalies in neonates with symptomatic CHD
Predicted probabilities of respiratory support at discharge based on birth weight, genetic diagnosis causative of CHD, and additional major congenital anomalies in neonates with symptomatic CHD Model 1 using birth weight, genetic diagnosis, and additional major congenital anomaly.
Model 1 using birth weight, genetic diagnosis, and additional major congenital anomaly. 