
Neonatal Hemodynamics and Cardiovascular Medicine 3
Session: Neonatal Hemodynamics and Cardiovascular Medicine 3

Mahati Pidaparti, MD
Fellow
Indiana University School of Medicine
Indianapolis, Indiana, United States
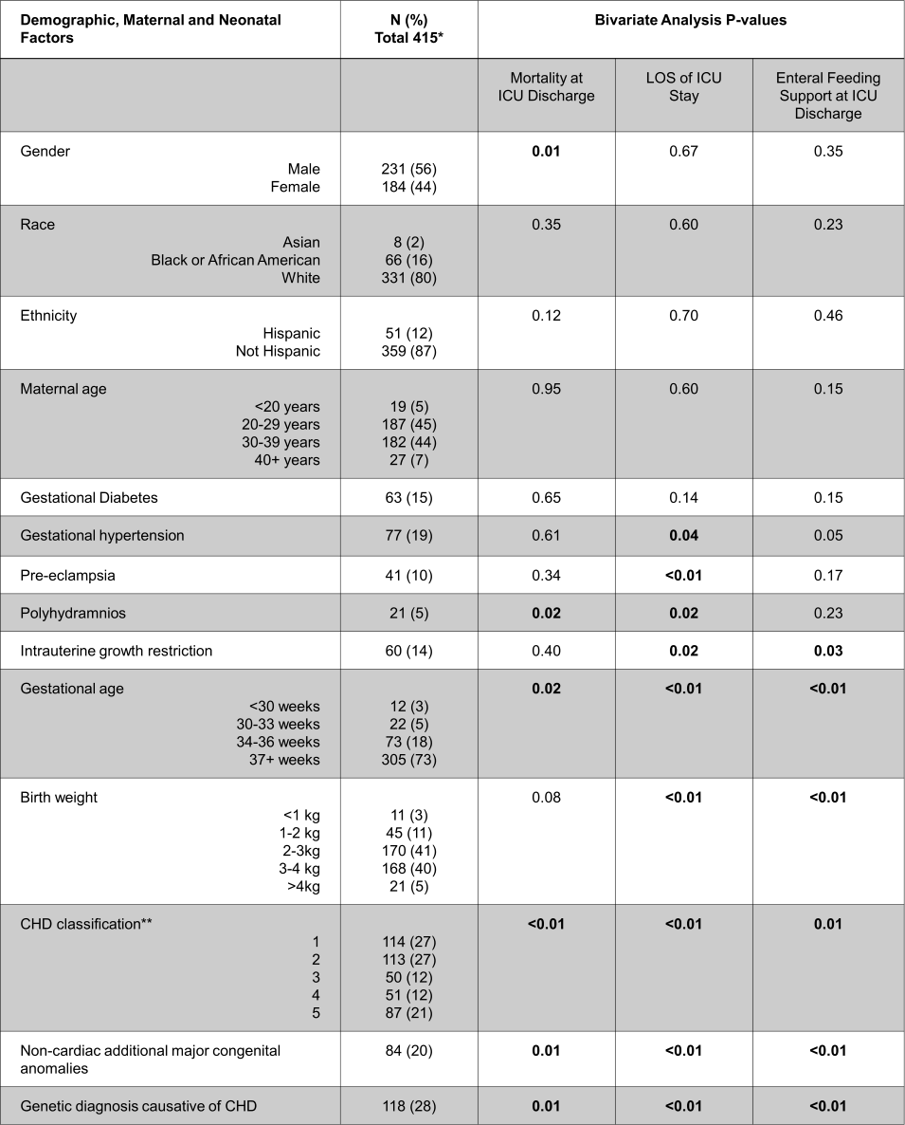 Bivariate analysis was performed using Chi-square and Fisher's Exact Tests for categorical variables (mortality and enteral feeding support at discharge) and Kruskal-Wallis for continuous variables (LOS).
Bivariate analysis was performed using Chi-square and Fisher's Exact Tests for categorical variables (mortality and enteral feeding support at discharge) and Kruskal-Wallis for continuous variables (LOS).