
Technology 1: AI/Machine Learning
Session: Technology 1: AI/Machine Learning

Ben Shank, MS, EMT-LP
CEO
EMx Biotech
Austin, Texas, United States
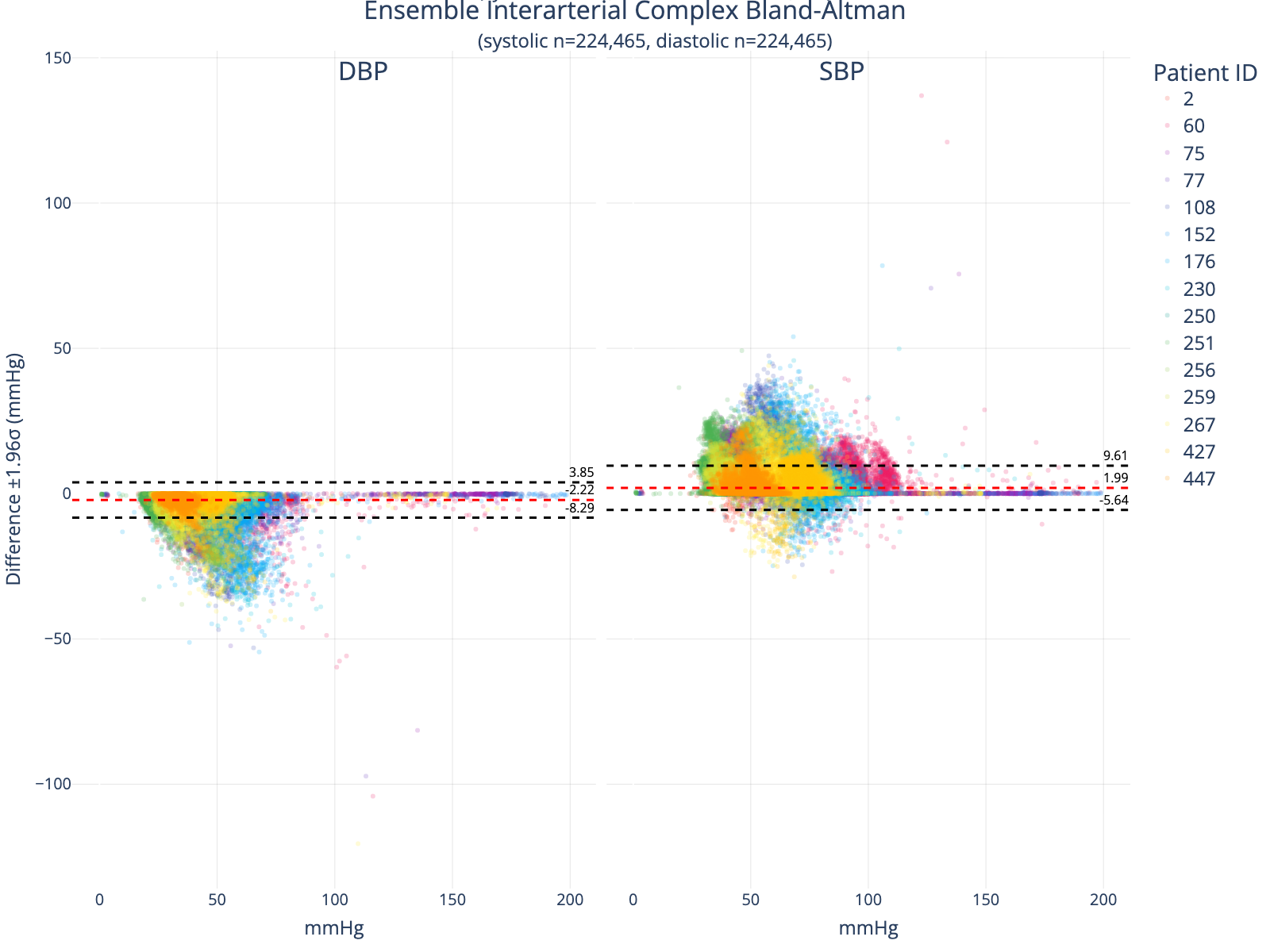 Bland-Altman Comparing True to Generated Arterial Complexes. This analysis excludes interarterial complexes that could not be matched due to ground truth waveform signal noise, nonperfusing arterial beats, or model predictions that could not be aligned to a true peak.
Bland-Altman Comparing True to Generated Arterial Complexes. This analysis excludes interarterial complexes that could not be matched due to ground truth waveform signal noise, nonperfusing arterial beats, or model predictions that could not be aligned to a true peak.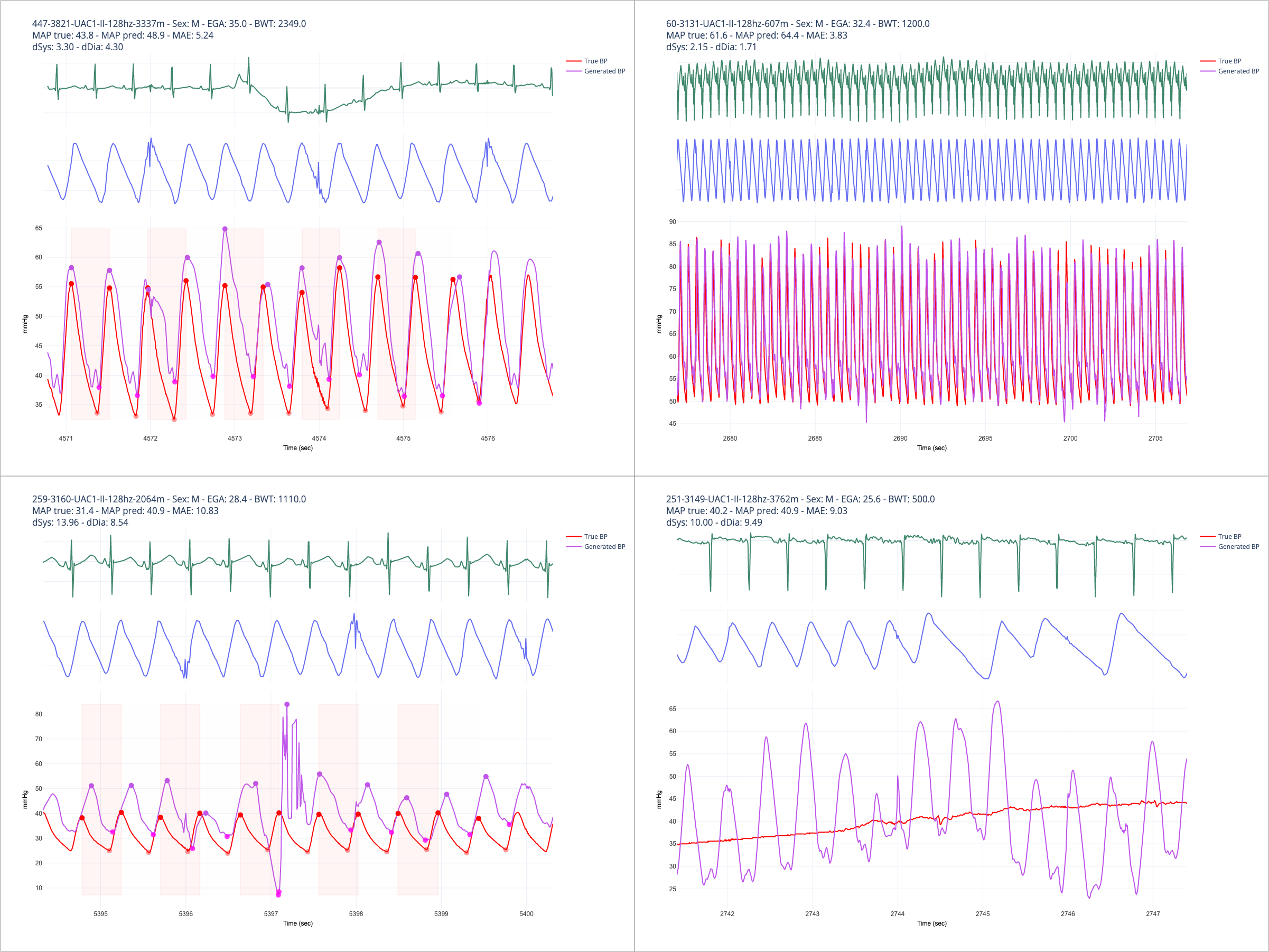 Random output traces at various levels of detail for different patients. The upper-right panel shows a relatively clean set of input signals and good concordance between true and predicted waveforms. The upper-left depicts error in the presence of ECG and PPG signal artifacts. Note the extremely erroneous prediction in the lower-left panel, which was an output pattern observed intermittently and caused by overfitting to noisy training data and insufficient regularization. The lower-right panel depicts an example that should typically be excluded from a machine learning training workflow, as the ground truth signal is corrupted.
Random output traces at various levels of detail for different patients. The upper-right panel shows a relatively clean set of input signals and good concordance between true and predicted waveforms. The upper-left depicts error in the presence of ECG and PPG signal artifacts. Note the extremely erroneous prediction in the lower-left panel, which was an output pattern observed intermittently and caused by overfitting to noisy training data and insufficient regularization. The lower-right panel depicts an example that should typically be excluded from a machine learning training workflow, as the ground truth signal is corrupted.