
Emergency Medicine 14
Session: Emergency Medicine 14
 photo")
Michelle R. Khattri, BS (she/her/hers)
Medical Student
Renaissance School of Medicine at Stony Brook University
Port Jefferson Station, New York, United States
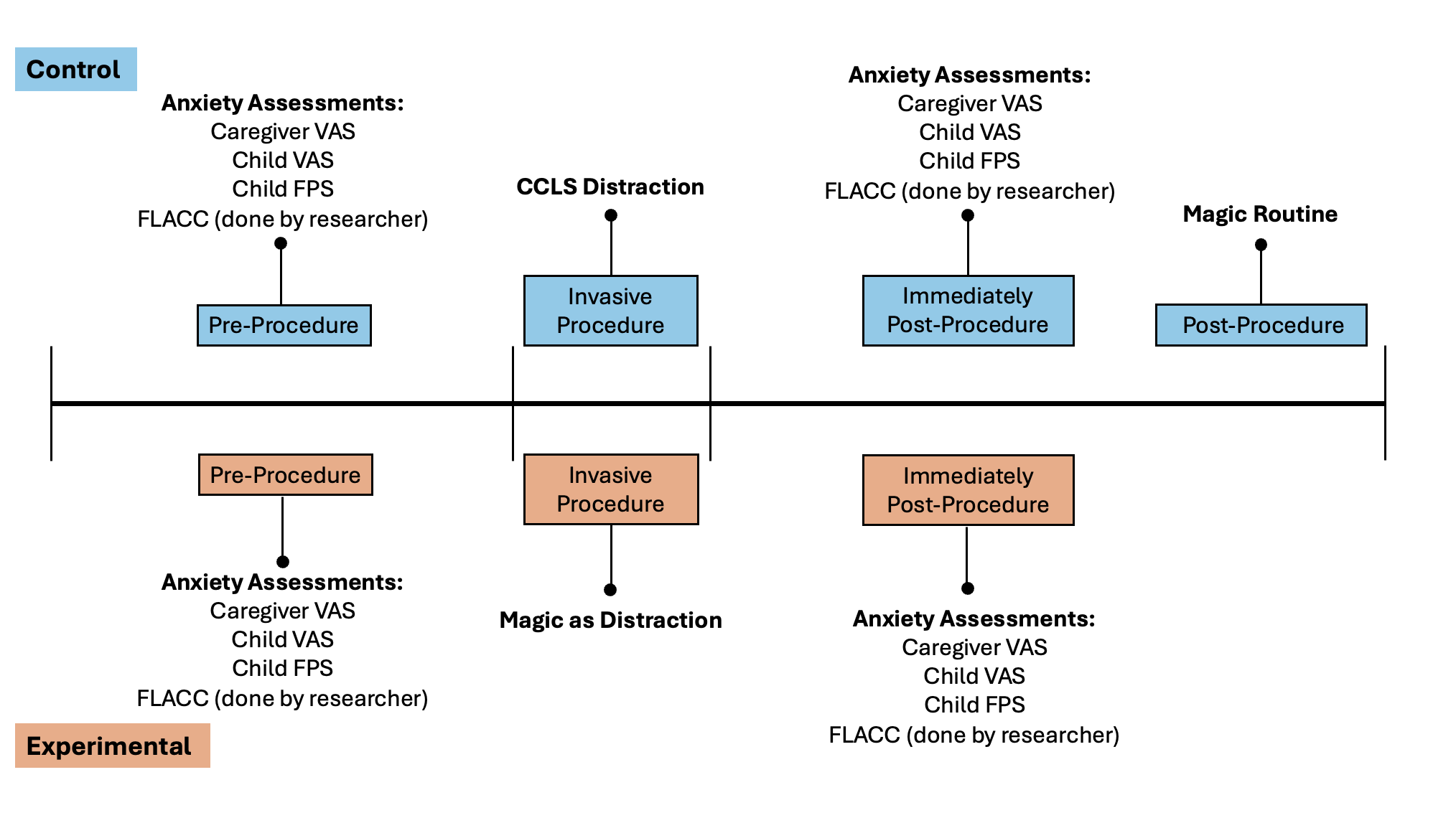 Anxiety assessment tools were completed pre-procedure and again immediately post-procedure. Standard CCLS distractions were done during the invasive procedure for the control group (blue), and magic distraction was done during the invasive procedure for the experimental group (red). A magic routine was still performed for patients in the control group after the needed anxiety metrics were obtained.
Anxiety assessment tools were completed pre-procedure and again immediately post-procedure. Standard CCLS distractions were done during the invasive procedure for the control group (blue), and magic distraction was done during the invasive procedure for the experimental group (red). A magic routine was still performed for patients in the control group after the needed anxiety metrics were obtained.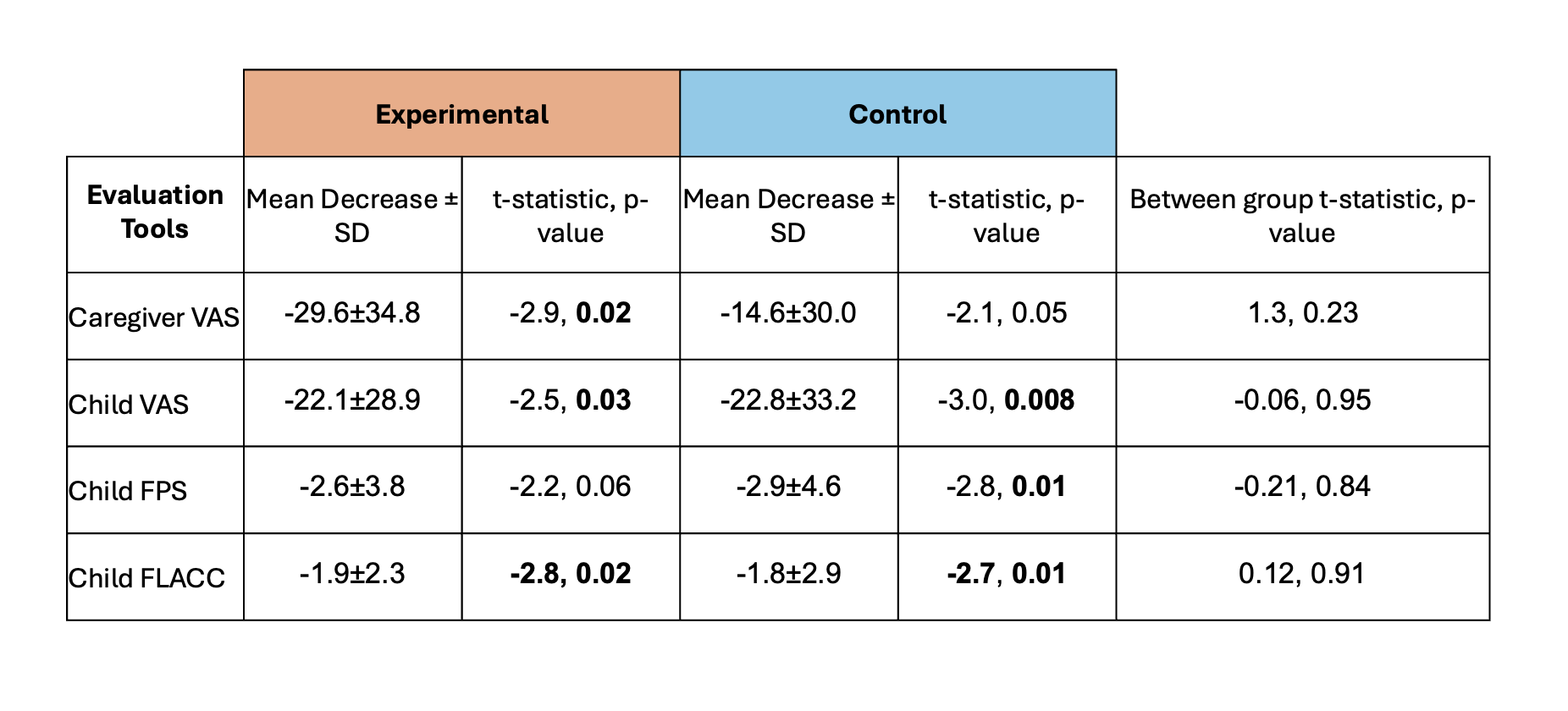 Average anxiety scores for all evaluation tools in both experimental and control groups. Within-group comparisons were assessed by paired two-tailed t-tests; between-group comparisons were assessed by two-sample two-tailed t-tests. P values < 0.05 were considered statistically significant and are highlighted in bold.
Average anxiety scores for all evaluation tools in both experimental and control groups. Within-group comparisons were assessed by paired two-tailed t-tests; between-group comparisons were assessed by two-sample two-tailed t-tests. P values < 0.05 were considered statistically significant and are highlighted in bold.